










Aim:
Transthoracic echocardiography (TTE) is the first-line imaging test for patients with chronic coronary syndrome (CCS) and the cornerstone of risk stratification is left ventricular (LV) ejection fraction (EF). Aim of the study was to investigate the value of TTE supplemented with strain echocardiography (STE) and lung ultrasound (LUS) to assess the risk of patients with CCS.
Methods:
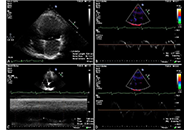
In a prospective, single-center, observational study, from November 2020 to December 2022, 529 consecutive patients with CCS were recruited. All patients were evaluated at rest. A single vendor machine (GE Vivid E95) was used. EF with biplane Simpson’s method (abnormal cut-off < 50%), LV global longitudinal strain (GLS%, abnormal cut-off ≤ 16.2% by receiver-operating characteristics analysis) by STE, and B-line score (abnormal cut-off ≥ 2) by LUS (4-site simplified scan) were assessed. Integrated TTE score ranged from 0 (all 3 parameters normal) to 3 (all parameters abnormal). All patients were followed-up and a composite endpoint was considered, including all-cause death, acute coronary syndrome (ACS), and myocardial revascularization.
Results:
During a follow-up of 14.2 months ± 8.3 months, 72 events occurred: 10 deaths, 11 ACSs, and 51 myocardial revascularizations. In multivariable analysis, B lines [hazard ratio (HR) 1.76, 95% confidence Interval (CI) 1.05–2.97; P = 0.03], and GLS ≤ 16.2% (HR 2.0, 95% CI 1.17–3.45; P = 0.01) were independent predictors of events. EF < 50% was a significant predictor in univariate, but not in multivariable analysis. Event rate at 2 years increased from score 0 (8%), to score 1 (21%), 2 (23%), and 3 (40%), P < 0.0001.
Conclusions:
TTE with left ventricular ejection fraction (LVEF) can be usefully integrated with STE for GLS, and LUS for B-lines, for better prediction of outcome in CCS. The 3 parameters can be obtained in every echo lab with basic technology, no harm, no risk, and no stress.
Aim:
Transthoracic echocardiography (TTE) is the first-line imaging test for patients with chronic coronary syndrome (CCS) and the cornerstone of risk stratification is left ventricular (LV) ejection fraction (EF). Aim of the study was to investigate the value of TTE supplemented with strain echocardiography (STE) and lung ultrasound (LUS) to assess the risk of patients with CCS.
Methods:
In a prospective, single-center, observational study, from November 2020 to December 2022, 529 consecutive patients with CCS were recruited. All patients were evaluated at rest. A single vendor machine (GE Vivid E95) was used. EF with biplane Simpson’s method (abnormal cut-off < 50%), LV global longitudinal strain (GLS%, abnormal cut-off ≤ 16.2% by receiver-operating characteristics analysis) by STE, and B-line score (abnormal cut-off ≥ 2) by LUS (4-site simplified scan) were assessed. Integrated TTE score ranged from 0 (all 3 parameters normal) to 3 (all parameters abnormal). All patients were followed-up and a composite endpoint was considered, including all-cause death, acute coronary syndrome (ACS), and myocardial revascularization.
Results:
During a follow-up of 14.2 months ± 8.3 months, 72 events occurred: 10 deaths, 11 ACSs, and 51 myocardial revascularizations. In multivariable analysis, B lines [hazard ratio (HR) 1.76, 95% confidence Interval (CI) 1.05–2.97; P = 0.03], and GLS ≤ 16.2% (HR 2.0, 95% CI 1.17–3.45; P = 0.01) were independent predictors of events. EF < 50% was a significant predictor in univariate, but not in multivariable analysis. Event rate at 2 years increased from score 0 (8%), to score 1 (21%), 2 (23%), and 3 (40%), P < 0.0001.
Conclusions:
TTE with left ventricular ejection fraction (LVEF) can be usefully integrated with STE for GLS, and LUS for B-lines, for better prediction of outcome in CCS. The 3 parameters can be obtained in every echo lab with basic technology, no harm, no risk, and no stress.
DOI: https://doi.org/10.37349/ec.2023.00007
The clinical manifestations of COVID-19 which mainly involve the respiratory system may however affect also cardiovascular system. There are a lot and still increasing numbers of reports revealing cardiovascular complications of COVID-19, which may occur in the acute phase as well as during longer follow-up period. The most clinically important diseases include: pulmonary embolism (PE), myocarditis, and acute coronary syndromes (ACS) as well as arrhythmias with the very common atrial fibrillation (AF) and pericarditis. In this review, cardiac imaging options in patients with and after coronavirus infection are presented, showing potential utility for expanding and improving the full and accurate diagnosis of potential complications. Echocardiography, magnetic resonance imaging, and computed tomography (CT) are considered in turn, highlighting their best advantages in patients affected by COVID.
The clinical manifestations of COVID-19 which mainly involve the respiratory system may however affect also cardiovascular system. There are a lot and still increasing numbers of reports revealing cardiovascular complications of COVID-19, which may occur in the acute phase as well as during longer follow-up period. The most clinically important diseases include: pulmonary embolism (PE), myocarditis, and acute coronary syndromes (ACS) as well as arrhythmias with the very common atrial fibrillation (AF) and pericarditis. In this review, cardiac imaging options in patients with and after coronavirus infection are presented, showing potential utility for expanding and improving the full and accurate diagnosis of potential complications. Echocardiography, magnetic resonance imaging, and computed tomography (CT) are considered in turn, highlighting their best advantages in patients affected by COVID.
DOI: https://doi.org/10.37349/ec.2023.00008
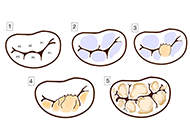
Mitral valve prolapse (MVP) is a relatively common mitral valvulopathy and the most common cause of isolated primary mitral regurgitation (MR) requiring surgical repair. It affects about 1–3% of the general population. Although MVP is viewed as a benign condition, the association between MVP and sudden cardiac death (SCD) has been proven. Patients with MVP have a three times higher risk of SCD than the general population. The underlying mechanisms and predictors of arrhythmias, which occur in patients with MVP, are still poorly understood. However, some echocardiographic features such as mitral annulus disjunction (MAD), bileaflet MVP (biMVP), and papillary muscle (PM) fibrosis were frequently linked with increased number of arrhythmic events and are referred to as “arrhythmogenic” or “malignant”. Arrhythmogenic MVP (AMVP) has also been associated with other factors such as female sex, polymorphic premature ventricular contraction (PVC), abnormalities of T-waves, and Pickelhaube sign on tissue Doppler tracing of the lateral part of the mitral annulus. Cardiac magnetic resonance (CMR) imaging and speckle tracking echocardiography are new tools showing significant potential for detection of malignant features of AMVP. This paper presents various data coming from electrocardiography (ECG) analysis, echocardiography, and other imaging techniques as well as compilation of the recent studies on the subject of MVP.
Mitral valve prolapse (MVP) is a relatively common mitral valvulopathy and the most common cause of isolated primary mitral regurgitation (MR) requiring surgical repair. It affects about 1–3% of the general population. Although MVP is viewed as a benign condition, the association between MVP and sudden cardiac death (SCD) has been proven. Patients with MVP have a three times higher risk of SCD than the general population. The underlying mechanisms and predictors of arrhythmias, which occur in patients with MVP, are still poorly understood. However, some echocardiographic features such as mitral annulus disjunction (MAD), bileaflet MVP (biMVP), and papillary muscle (PM) fibrosis were frequently linked with increased number of arrhythmic events and are referred to as “arrhythmogenic” or “malignant”. Arrhythmogenic MVP (AMVP) has also been associated with other factors such as female sex, polymorphic premature ventricular contraction (PVC), abnormalities of T-waves, and Pickelhaube sign on tissue Doppler tracing of the lateral part of the mitral annulus. Cardiac magnetic resonance (CMR) imaging and speckle tracking echocardiography are new tools showing significant potential for detection of malignant features of AMVP. This paper presents various data coming from electrocardiography (ECG) analysis, echocardiography, and other imaging techniques as well as compilation of the recent studies on the subject of MVP.
DOI: https://doi.org/10.37349/ec.2023.00009
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin
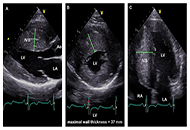
The use of echocardiography, a straightforward and widely available technique, allows for a comprehensive assessment of the patient with hypertrophic cardiomyopathy (HCM) under both resting and stress conditions. The true prevalence of HCM has been redefined over time by this imaging approach, which has also made it feasible to pinpoint parameters that clinicians may use to stratify patients at risk for adverse cardiovascular events. The current and emerging prognostic predictors in HCM, assessed with transthoracic echocardiography at rest and during provocation, are discussed in this review.
The use of echocardiography, a straightforward and widely available technique, allows for a comprehensive assessment of the patient with hypertrophic cardiomyopathy (HCM) under both resting and stress conditions. The true prevalence of HCM has been redefined over time by this imaging approach, which has also made it feasible to pinpoint parameters that clinicians may use to stratify patients at risk for adverse cardiovascular events. The current and emerging prognostic predictors in HCM, assessed with transthoracic echocardiography at rest and during provocation, are discussed in this review.
DOI: https://doi.org/10.37349/ec.2023.00010
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin
Aim:
Transthoracic echocardiography is commonly used to assess coronary artery dilatation in Kawasaki disease (KD). However, existing criteria often miss early abnormalities. This study examines the utility of a new parameter, coronary external diameter index (CEDi), for early diagnosis and monitoring in KD.
Methods:
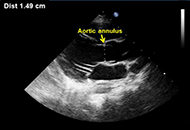
CEDi of left main (LM) and right coronary artery (RCA), calculated as the ratio of coronary artery external diameter (i.e., the distance between the outer coronary edges measured in the proximal segment of the artery) and the diameter of the aortic annulus, was evaluated in 34 patients (age 23 mouths ± 13 months) with KD at the hospital admission and after 2 weeks and 8 weeks of treatment. The control group consisted of 210 healthy children aged 20 months ± 13.4 months. Z-score charts for LM and RCA coronary external diameter (CED) were obtained.
Results:
Compared with controls, KD patients had a markedly higher mean value of LM CEDi (0.53 ± 0.06 vs. 0.33 ± 0.04; P < 0.0001) and RCA CEDi (0.48 ± 0.05 vs. 0.31 ± 0.04; P < 0.0001) at hospital admission. By ROC analysis, LM CEDi of 0.41, and RCA coronary artery thickness index (CATi) of 0.39 were the best cut-offs to confirm the clinical diagnosis of KD, both exhibiting 100% sensitivity and specificity. Mean LM CEDi and RCA CEDi values decreased significantly (P < 0.0001) after 2 weeks of follow-up and were similar to controls (P = 0.53 and P = 0.12, respectively) 8 weeks after admission.
Conclusions:
In patients with KD, CEDi of LM and RCA is an accurate parameter to evaluate coronary artery involvement in the early phase of the illness and during follow-up.
Aim:
Transthoracic echocardiography is commonly used to assess coronary artery dilatation in Kawasaki disease (KD). However, existing criteria often miss early abnormalities. This study examines the utility of a new parameter, coronary external diameter index (CEDi), for early diagnosis and monitoring in KD.
Methods:
CEDi of left main (LM) and right coronary artery (RCA), calculated as the ratio of coronary artery external diameter (i.e., the distance between the outer coronary edges measured in the proximal segment of the artery) and the diameter of the aortic annulus, was evaluated in 34 patients (age 23 mouths ± 13 months) with KD at the hospital admission and after 2 weeks and 8 weeks of treatment. The control group consisted of 210 healthy children aged 20 months ± 13.4 months. Z-score charts for LM and RCA coronary external diameter (CED) were obtained.
Results:
Compared with controls, KD patients had a markedly higher mean value of LM CEDi (0.53 ± 0.06 vs. 0.33 ± 0.04; P < 0.0001) and RCA CEDi (0.48 ± 0.05 vs. 0.31 ± 0.04; P < 0.0001) at hospital admission. By ROC analysis, LM CEDi of 0.41, and RCA coronary artery thickness index (CATi) of 0.39 were the best cut-offs to confirm the clinical diagnosis of KD, both exhibiting 100% sensitivity and specificity. Mean LM CEDi and RCA CEDi values decreased significantly (P < 0.0001) after 2 weeks of follow-up and were similar to controls (P = 0.53 and P = 0.12, respectively) 8 weeks after admission.
Conclusions:
In patients with KD, CEDi of LM and RCA is an accurate parameter to evaluate coronary artery involvement in the early phase of the illness and during follow-up.
DOI: https://doi.org/10.37349/ec.2023.00011
Congenital heart defects (CHD) represent the most frequent congenital anomalies among newborns, as well as the leading cause of spontaneous abortion, stillbirth, neonatal and infant death. CHD have been recognized as multifactorial diseases, with environmental contaminants as potential contributors to the etiopathogenesis of CHD. Toxic elements, such as arsenic (As), cadmium (Cd), lead (Pb), and mercury (Hg) are known to be associated with adverse reproductive outcomes and certain congenital anomalies, however their association with the risk for CHD remains inconsistent. This review summarizes the updated evidence on the CHD-associated risk related to exposure to As, Cd, Hg, Pb during pregnancy, reporting the main findings from epidemiological and experimental studies and the underlying molecular mechanisms. Additionally, being diet the major source of these elements in the general population, after having identified the main vectors of toxic metals in food, possible remediation strategies to reduce diet-related risks are also described. Among these, a novel, consumer-centered approach in developing new foods is discussed, considering not only the nutritional characteristics of edible compounds foods are made up of, but also their organoleptic features, making the food even more appealing to the consumer. Overall, current data support the association of maternal exposure to As and Pb with increased risk for CHD, although significant associations have only been observed for total and/or specific subgroups. On the other hand, the evidence of association for Cd and Hg exposure in pregnancy with CHD in the offspring remains, yet, quite speculative. Further large prospective cohort studies and insights into the molecular and biomolecular processes of these relationships are warranted to further explore and/or verify these findings.
Congenital heart defects (CHD) represent the most frequent congenital anomalies among newborns, as well as the leading cause of spontaneous abortion, stillbirth, neonatal and infant death. CHD have been recognized as multifactorial diseases, with environmental contaminants as potential contributors to the etiopathogenesis of CHD. Toxic elements, such as arsenic (As), cadmium (Cd), lead (Pb), and mercury (Hg) are known to be associated with adverse reproductive outcomes and certain congenital anomalies, however their association with the risk for CHD remains inconsistent. This review summarizes the updated evidence on the CHD-associated risk related to exposure to As, Cd, Hg, Pb during pregnancy, reporting the main findings from epidemiological and experimental studies and the underlying molecular mechanisms. Additionally, being diet the major source of these elements in the general population, after having identified the main vectors of toxic metals in food, possible remediation strategies to reduce diet-related risks are also described. Among these, a novel, consumer-centered approach in developing new foods is discussed, considering not only the nutritional characteristics of edible compounds foods are made up of, but also their organoleptic features, making the food even more appealing to the consumer. Overall, current data support the association of maternal exposure to As and Pb with increased risk for CHD, although significant associations have only been observed for total and/or specific subgroups. On the other hand, the evidence of association for Cd and Hg exposure in pregnancy with CHD in the offspring remains, yet, quite speculative. Further large prospective cohort studies and insights into the molecular and biomolecular processes of these relationships are warranted to further explore and/or verify these findings.
DOI: https://doi.org/10.37349/ec.2023.00012
This article belongs to the special issue Environmental Cardiology
DOI: https://doi.org/10.37349/ec.2023.00001
Aim:
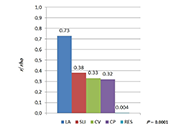
Left ventricular (LV) hypertrophy (LVH) is a common and relevant complication of arterial hypertension (AH) and 12-lead electrocardiogram (ECG) is widely used for its preliminary assessment. The aim of the study was to compare the correlations of four ECG-derived criteria of LVH and left atrial (LA) anteroposterior diameter with LVH assessed by echocardiography and expressed as left ventricular mass (LVM) index (LVMI) in search of the most accurate preliminary indicator of LVH.
Methods:
The study included 61 subjects with AH [age (year) 69 ± 10, 17 females] and 27 without AH, (age 40 ± 9, 10 females) evaluated with 12-lead ECG and transthoracic echocardiography (TTE). As the ECG-based criteria of LVH Sokolow-Lyon index (SLI), Cornell voltage (CV), Cornell product (CP), and Romhilt-Estes point score (RES) system were evaluated. The ECG indices and LA diameter were correlated with LVMI and correlations coefficients were compared.
Results:
Among ECG-LVH indicators SLI showed the closest correlation with LVMI [rank correlation coefficients (rho) = 0.38, P < 0.0001], followed by CV and CP with rho = 0.33, P = 0.002 and rho = 0.32, P = 0.002, respectively, whereas RES did not correlate significantly with LVMI. The strongest correlation with LVMI was found for the LA diameter with rho = 0.73 and P < 0.0001, showing an even stronger correlation in women—rho = 0.8 (P < 0.0001) vs. rho = 0.65 (P < 0.0001) in men. In the multivariate analysis, the LA was the only independent predictor of the increased LVMI with R2 = 0.52, P < 0.0001.
Conclusions:
LA diameter outperformed significantly the ECG indices as far as the correlation with LVMI was concerned and emerged as the only independent predictor of mild and moderate LVH in hypertensive patients. Among the ECG criteria, the strongest correlation was shown for SLI, followed by CV and CP indices.
Aim:
Left ventricular (LV) hypertrophy (LVH) is a common and relevant complication of arterial hypertension (AH) and 12-lead electrocardiogram (ECG) is widely used for its preliminary assessment. The aim of the study was to compare the correlations of four ECG-derived criteria of LVH and left atrial (LA) anteroposterior diameter with LVH assessed by echocardiography and expressed as left ventricular mass (LVM) index (LVMI) in search of the most accurate preliminary indicator of LVH.
Methods:
The study included 61 subjects with AH [age (year) 69 ± 10, 17 females] and 27 without AH, (age 40 ± 9, 10 females) evaluated with 12-lead ECG and transthoracic echocardiography (TTE). As the ECG-based criteria of LVH Sokolow-Lyon index (SLI), Cornell voltage (CV), Cornell product (CP), and Romhilt-Estes point score (RES) system were evaluated. The ECG indices and LA diameter were correlated with LVMI and correlations coefficients were compared.
Results:
Among ECG-LVH indicators SLI showed the closest correlation with LVMI [rank correlation coefficients (rho) = 0.38, P < 0.0001], followed by CV and CP with rho = 0.33, P = 0.002 and rho = 0.32, P = 0.002, respectively, whereas RES did not correlate significantly with LVMI. The strongest correlation with LVMI was found for the LA diameter with rho = 0.73 and P < 0.0001, showing an even stronger correlation in women—rho = 0.8 (P < 0.0001) vs. rho = 0.65 (P < 0.0001) in men. In the multivariate analysis, the LA was the only independent predictor of the increased LVMI with R2 = 0.52, P < 0.0001.
Conclusions:
LA diameter outperformed significantly the ECG indices as far as the correlation with LVMI was concerned and emerged as the only independent predictor of mild and moderate LVH in hypertensive patients. Among the ECG criteria, the strongest correlation was shown for SLI, followed by CV and CP indices.
DOI: https://doi.org/10.37349/ec.2023.00002
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin
The deleterious consequences of alcohol consumption are extensively documented across various dimensions of human health, encompassing somatic disorders such as nervous system impairments, digestive system abnormalities, and circulatory dysfunctions, in addition to socio-psychological aspects. Within the domain of cardiology, a substantial portion of the ongoing scientific discourse centers on elucidating the toxic dose of alcohol. Presented herewith are the findings from a comprehensive review of the latest publications pertinent to this crucial issue.
The deleterious consequences of alcohol consumption are extensively documented across various dimensions of human health, encompassing somatic disorders such as nervous system impairments, digestive system abnormalities, and circulatory dysfunctions, in addition to socio-psychological aspects. Within the domain of cardiology, a substantial portion of the ongoing scientific discourse centers on elucidating the toxic dose of alcohol. Presented herewith are the findings from a comprehensive review of the latest publications pertinent to this crucial issue.
DOI: https://doi.org/10.37349/ec.2023.00003
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin
Aim:
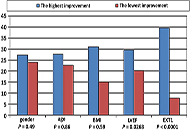
The aim of this study was to compare initial and final exercise tolerance and to evaluate the determinants of exercise capacity improvement—after three weeks of inpatient cardiac rehabilitation.
Methods:
A cohort of 494 patients after acute coronary syndrome (ACS), treated with primary coronary angioplasty (age 60 years ± 10 years, 27.5% women) was studied retrospectively. Possible correlations between improvement and age, gender, body mass index (BMI), left ventricular ejection fraction (LVEF) and the initial exercise capacity (EXT1) were assessed.
Results:
The highest percentage of patients with improvement (43.6%) was in the medium tercile of LVEF (> 42% but ≤ 50%) and was more likely in the medium tercile of initial exercise tolerance [> 5.7 but ≤ 8.4 metabolic equivalent of tasks (METs)]. Receiver-operator characteristic (ROC) curves were developed and the following cut-off values were found: for LVEF > 43% (this value had 69.6% sensitivity in predicting improvement; the chance of improvement was 2.67 higher than in patients with LVEF ≤ 43%); for EXT1 ≤ 8.4 METs (this value had 70.8% sensitivity, the chance of improvement was 1.86 higher than in the other subgroup). No significant relationship between improvement and gender, age or BMI was found.
Conclusions:
The combination of LVEF > 43% and EXT1 ≤ 8.4 METs relates to the highest probability of exercise tolerance improvement after cardiac rehabilitation.
Aim:
The aim of this study was to compare initial and final exercise tolerance and to evaluate the determinants of exercise capacity improvement—after three weeks of inpatient cardiac rehabilitation.
Methods:
A cohort of 494 patients after acute coronary syndrome (ACS), treated with primary coronary angioplasty (age 60 years ± 10 years, 27.5% women) was studied retrospectively. Possible correlations between improvement and age, gender, body mass index (BMI), left ventricular ejection fraction (LVEF) and the initial exercise capacity (EXT1) were assessed.
Results:
The highest percentage of patients with improvement (43.6%) was in the medium tercile of LVEF (> 42% but ≤ 50%) and was more likely in the medium tercile of initial exercise tolerance [> 5.7 but ≤ 8.4 metabolic equivalent of tasks (METs)]. Receiver-operator characteristic (ROC) curves were developed and the following cut-off values were found: for LVEF > 43% (this value had 69.6% sensitivity in predicting improvement; the chance of improvement was 2.67 higher than in patients with LVEF ≤ 43%); for EXT1 ≤ 8.4 METs (this value had 70.8% sensitivity, the chance of improvement was 1.86 higher than in the other subgroup). No significant relationship between improvement and gender, age or BMI was found.
Conclusions:
The combination of LVEF > 43% and EXT1 ≤ 8.4 METs relates to the highest probability of exercise tolerance improvement after cardiac rehabilitation.
DOI: https://doi.org/10.37349/ec.2023.00004
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin
Alcohol drinks, especially wine, have been described since 6,000 B.C. For many years in modern medicine, wine in moderation has been considered healthy for cardiovascular prevention, i.e., recommended by nutrition committees. Some regional guidelines still recommend one to two standard drinks per day. By the very recent (January 2023), World Health Organization and Canadian Guidance on alcohol emphasize that any alcoholic drink is hazardous to the health and the safe amount is zero. The risk starts with every single drop. It was also nicely summarized in the manuscript “Alcohol-dose question and the weakest link in a chemical interplay” (Explor Cardiol. 2023;1:15–25. doi: 10.37349/ec.2023.00003) especially from the standpoint of a researcher in the cardiovascular arena. The newest recommendations are based on observational studies and their meta-analysis, therefore establishing associations, pointing out that alcohol may somewhat prevent cardiovascular diseases and diabetes type 2, but with a significant increase in non-cardiovascular morbidity and mortality, especially cancers. Previous recommendations, therefore, may be obsolete as they were based on studies where abstainers from alcoholic beverages had inherent higher risks. The current controversy with conflicting guidelines for alcoholic beverage consumption in the era of precision medicine may stimulate more fundamental investigations up to genetic ones and find the cause-effect relations. In the era of precision medicine, it may come closer to discovering the causes of cancers and many other diseases, enabling predictions of reactions to alcoholic beverages by each person, not just in the population.
Alcohol drinks, especially wine, have been described since 6,000 B.C. For many years in modern medicine, wine in moderation has been considered healthy for cardiovascular prevention, i.e., recommended by nutrition committees. Some regional guidelines still recommend one to two standard drinks per day. By the very recent (January 2023), World Health Organization and Canadian Guidance on alcohol emphasize that any alcoholic drink is hazardous to the health and the safe amount is zero. The risk starts with every single drop. It was also nicely summarized in the manuscript “Alcohol-dose question and the weakest link in a chemical interplay” (Explor Cardiol. 2023;1:15–25. doi: 10.37349/ec.2023.00003) especially from the standpoint of a researcher in the cardiovascular arena. The newest recommendations are based on observational studies and their meta-analysis, therefore establishing associations, pointing out that alcohol may somewhat prevent cardiovascular diseases and diabetes type 2, but with a significant increase in non-cardiovascular morbidity and mortality, especially cancers. Previous recommendations, therefore, may be obsolete as they were based on studies where abstainers from alcoholic beverages had inherent higher risks. The current controversy with conflicting guidelines for alcoholic beverage consumption in the era of precision medicine may stimulate more fundamental investigations up to genetic ones and find the cause-effect relations. In the era of precision medicine, it may come closer to discovering the causes of cancers and many other diseases, enabling predictions of reactions to alcoholic beverages by each person, not just in the population.
DOI: https://doi.org/10.37349/ec.2023.00005
Aim:
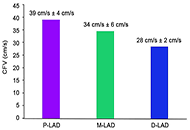
Coronary flow velocity (CFV) can be obtained with transthoracic echocardiography (TTE) in the left anterior descending coronary artery (LAD). The physiologic flow velocity gradient across the different segments of LAD has not been established. This study aims to assess the normal values of resting CFV in proximal, mid, and distal LAD.
Methods:
In a single center, prospective, observational study design, TTE was attempted on 110 consecutive, asymptomatic middle-aged subjects (age = 55 years, 46% males) with a low likelihood of coronary artery disease (< 5%). Resting CFV in the LAD was assessed with high-end machines, dedicated coronary pre-set, and high-frequency transducers by pulsed-wave Doppler under color-Doppler guidance in the proximal, mid, and distal segments.
Results:
The technical success rate for CFV imaging was lowest for the proximal (101/110, 92%), intermediate for mid (106/110, 96%), and highest for the distal segment (108/110, 98%). All 3 segments were interpretable in 101 subjects. CFV was highest in proximal segments (38.6 cm/s ± 3.9 cm/s), intermediate in mid segments (34.3 cm/s ± 6.04 cm/s, P < 0.01 vs. proximal), and lowest in distal segments (28.1 cm/s ± 1.7 cm/s, P < 0.01 vs. proximal and vs. mid).
Conclusions:
A resting evaluation of CFV-LAD can be obtained by TTE in the large majority of consecutive subjects referred to the echocardiography laboratory. Feasibility is highest for distal and lowest for proximal-LAD segments. There is a clear physiologic gradient of CFV with decreasing values, of about 10% for each step, going from proximal to mid and distal segments of LAD. When resting CFV is considered, the site of the sampling is important to obtain comparable and physiologically meaningful data.
Aim:
Coronary flow velocity (CFV) can be obtained with transthoracic echocardiography (TTE) in the left anterior descending coronary artery (LAD). The physiologic flow velocity gradient across the different segments of LAD has not been established. This study aims to assess the normal values of resting CFV in proximal, mid, and distal LAD.
Methods:
In a single center, prospective, observational study design, TTE was attempted on 110 consecutive, asymptomatic middle-aged subjects (age = 55 years, 46% males) with a low likelihood of coronary artery disease (< 5%). Resting CFV in the LAD was assessed with high-end machines, dedicated coronary pre-set, and high-frequency transducers by pulsed-wave Doppler under color-Doppler guidance in the proximal, mid, and distal segments.
Results:
The technical success rate for CFV imaging was lowest for the proximal (101/110, 92%), intermediate for mid (106/110, 96%), and highest for the distal segment (108/110, 98%). All 3 segments were interpretable in 101 subjects. CFV was highest in proximal segments (38.6 cm/s ± 3.9 cm/s), intermediate in mid segments (34.3 cm/s ± 6.04 cm/s, P < 0.01 vs. proximal), and lowest in distal segments (28.1 cm/s ± 1.7 cm/s, P < 0.01 vs. proximal and vs. mid).
Conclusions:
A resting evaluation of CFV-LAD can be obtained by TTE in the large majority of consecutive subjects referred to the echocardiography laboratory. Feasibility is highest for distal and lowest for proximal-LAD segments. There is a clear physiologic gradient of CFV with decreasing values, of about 10% for each step, going from proximal to mid and distal segments of LAD. When resting CFV is considered, the site of the sampling is important to obtain comparable and physiologically meaningful data.
DOI: https://doi.org/10.37349/ec.2023.00006
Aim:
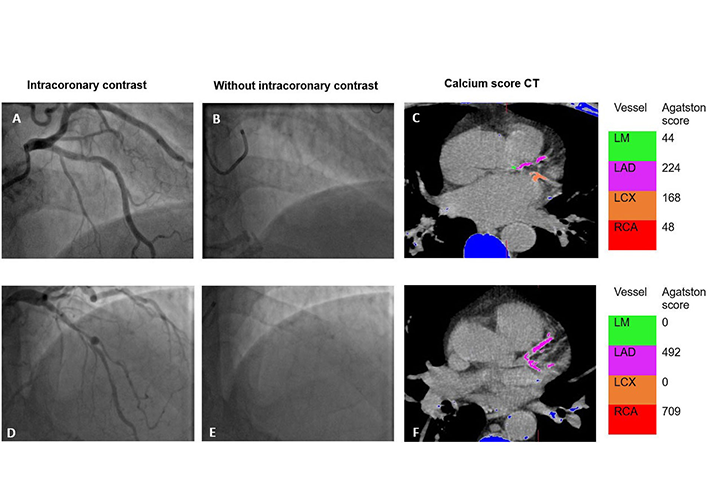
The pattern and severity of coronary artery calcification (CAC) can influence prognosis and outcome in percutaneous coronary intervention. An objective assessment of CAC during invasive angiography may provide additional prognostic information. This study aimed to assess the correlation between the angiographic Birmingham calcium score (BCS) and the Agatston coronary calcium score (CCS) performed as part of single-photon emission computed tomography myocardial perfusion imaging (SPECT-MPI).
Methods:
In this retrospective observational study, patients undergoing SPECT-MPI and invasive coronary angiography as part of their routine management were included. BCS was calculated by reviewing angiography images in retrospect by an observer blinded to the SPECT-MPI calcium score. Spearman’s correlation was used to analyze the correlation between BCS and SPECT-MPI. Receiver operating characteristic curve was used to detect cut-off for BCS that would detect clinically significant CAC [> 400 Agatston units (AU)]. Kaplan-Meier was used to report on outcomes at 5 years follow-up.
Results:
In this cohort of 151 patients, there was a positive correlation between BCS and CCS [Spearman correlation coefficient (r) = 0.558, P < 0.001]. Cumulative BCS of 1 was able to identify clinically significant CAC [area under the curve 0.788, 95% confidence interval (CI) 0.714–0.863]. Cumulative BCS ≥ 3 was associated with major adverse outcomes at 5 years follow-up (log rank P = 0.013).
Conclusion:
BCS correlates well with established higher CCS. Application of BCS during invasive coronary angiography will aid risk stratification, management, and follow-up with no extra patient involvement, radiation, or costs.
Aim:
The pattern and severity of coronary artery calcification (CAC) can influence prognosis and outcome in percutaneous coronary intervention. An objective assessment of CAC during invasive angiography may provide additional prognostic information. This study aimed to assess the correlation between the angiographic Birmingham calcium score (BCS) and the Agatston coronary calcium score (CCS) performed as part of single-photon emission computed tomography myocardial perfusion imaging (SPECT-MPI).
Methods:
In this retrospective observational study, patients undergoing SPECT-MPI and invasive coronary angiography as part of their routine management were included. BCS was calculated by reviewing angiography images in retrospect by an observer blinded to the SPECT-MPI calcium score. Spearman’s correlation was used to analyze the correlation between BCS and SPECT-MPI. Receiver operating characteristic curve was used to detect cut-off for BCS that would detect clinically significant CAC [> 400 Agatston units (AU)]. Kaplan-Meier was used to report on outcomes at 5 years follow-up.
Results:
In this cohort of 151 patients, there was a positive correlation between BCS and CCS [Spearman correlation coefficient (r) = 0.558, P < 0.001]. Cumulative BCS of 1 was able to identify clinically significant CAC [area under the curve 0.788, 95% confidence interval (CI) 0.714–0.863]. Cumulative BCS ≥ 3 was associated with major adverse outcomes at 5 years follow-up (log rank P = 0.013).
Conclusion:
BCS correlates well with established higher CCS. Application of BCS during invasive coronary angiography will aid risk stratification, management, and follow-up with no extra patient involvement, radiation, or costs.
DOI: https://doi.org/10.37349/ec.2024.00022
Drawing insights from a spectrum of in vitro, in vivo experimental, and clinical studies, this review illuminates the underlying mechanism by which iodinated contrast media (ICM) exerts an indirect genotoxic effect. The mechanism involves the photoelectric effect induced by iodine molecules, thereby augmenting radiation attenuation and subsequently elevating the locally absorbed radiation dose. The ensuing generation of secondary electrons from each photoelectric absorption interaction triggers molecular reactions, culminating in discernible DNA damage, notably in the form of DNA double-strand breaks. A convergence of evidence from in vitro, experimental, and clinical investigations underscores a consistent pattern: the addition of iodine contrast linearly heightens the absorbed radiation dose and associated DNA damage. This quantification was evident through alterations in attenuation and the manifestation of double-strand breaks in circulating lymphocytes, serving as an intermediate endpoint and a potential long-term indicator of cancer. The observed surplus of DNA damage in contrast-enhanced images compared to non-contrast images ranged notably from +30% to +200%. This broad range accentuates a substantial amplification effect on radiation-induced damage, particularly noteworthy at clinically relevant iodine doses. Crucially, this effect remains unaffected by brands or manufacturers and exhibits a robust, exclusive correlation with the concentration of iodine in the bloodstream. The significant augmentation of absorbed dose and genotoxic impact of X-rays due to the use of contrast agents warrants critical attention within the medical community. This often-unacknowledged genotoxic influence may play a pivotal role in elevating cancer risks among patients undergoing radiation-based procedures, necessitating a reconsideration of risk assessment protocols and clinical practices.
Drawing insights from a spectrum of in vitro, in vivo experimental, and clinical studies, this review illuminates the underlying mechanism by which iodinated contrast media (ICM) exerts an indirect genotoxic effect. The mechanism involves the photoelectric effect induced by iodine molecules, thereby augmenting radiation attenuation and subsequently elevating the locally absorbed radiation dose. The ensuing generation of secondary electrons from each photoelectric absorption interaction triggers molecular reactions, culminating in discernible DNA damage, notably in the form of DNA double-strand breaks. A convergence of evidence from in vitro, experimental, and clinical investigations underscores a consistent pattern: the addition of iodine contrast linearly heightens the absorbed radiation dose and associated DNA damage. This quantification was evident through alterations in attenuation and the manifestation of double-strand breaks in circulating lymphocytes, serving as an intermediate endpoint and a potential long-term indicator of cancer. The observed surplus of DNA damage in contrast-enhanced images compared to non-contrast images ranged notably from +30% to +200%. This broad range accentuates a substantial amplification effect on radiation-induced damage, particularly noteworthy at clinically relevant iodine doses. Crucially, this effect remains unaffected by brands or manufacturers and exhibits a robust, exclusive correlation with the concentration of iodine in the bloodstream. The significant augmentation of absorbed dose and genotoxic impact of X-rays due to the use of contrast agents warrants critical attention within the medical community. This often-unacknowledged genotoxic influence may play a pivotal role in elevating cancer risks among patients undergoing radiation-based procedures, necessitating a reconsideration of risk assessment protocols and clinical practices.
DOI: https://doi.org/10.37349/ec.2024.00023
While authorship practices can vary across different disciplines, authorship should reflect the individuals who have made a substantial contribution to the research project, take public responsibility for the paper’s content, and agree to its submission for publication. In real life, the article is usually authored by at least one truly genuine author and some parasitic authors. The first author and the last author are especially important. The middle authors are less important, and their participation is often wrongly seen as an inconsequential decorative favor. The honorary author, a gift or guest author, is added as a bonus to please someone higher in the hierarchy than the submitting author. This practice is believed to enhance the chances of publication, but usually, the excess of honorary authors will make reviewers more critical. A ghost author contributed substantially but it does not appear in the list of authors to avoid declaring an overt conflict of interest. The gold author is someone paid by a third party in direct or indirect forms, and capable of writing and signing everything asked by the payer, including overstating the merits of a new drug or ignoring its drawbacks. A fake author does not exist, and while it may seem humorous it is a breach of scientific integrity and can lead to serious consequences for the individuals involved. With Chat-generative pre-trained transformer (Chat-GPT), artificial intelligence may contribute decisively to the article content and presentation. Overall, it is important to maintain high standards of integrity and transparency in authorship practices to ensure that research findings are trustworthy and reliable. The reputation of your work is in the hands of your coauthors, so choose them carefully and make sure they share your commitment to scientific integrity.
While authorship practices can vary across different disciplines, authorship should reflect the individuals who have made a substantial contribution to the research project, take public responsibility for the paper’s content, and agree to its submission for publication. In real life, the article is usually authored by at least one truly genuine author and some parasitic authors. The first author and the last author are especially important. The middle authors are less important, and their participation is often wrongly seen as an inconsequential decorative favor. The honorary author, a gift or guest author, is added as a bonus to please someone higher in the hierarchy than the submitting author. This practice is believed to enhance the chances of publication, but usually, the excess of honorary authors will make reviewers more critical. A ghost author contributed substantially but it does not appear in the list of authors to avoid declaring an overt conflict of interest. The gold author is someone paid by a third party in direct or indirect forms, and capable of writing and signing everything asked by the payer, including overstating the merits of a new drug or ignoring its drawbacks. A fake author does not exist, and while it may seem humorous it is a breach of scientific integrity and can lead to serious consequences for the individuals involved. With Chat-generative pre-trained transformer (Chat-GPT), artificial intelligence may contribute decisively to the article content and presentation. Overall, it is important to maintain high standards of integrity and transparency in authorship practices to ensure that research findings are trustworthy and reliable. The reputation of your work is in the hands of your coauthors, so choose them carefully and make sure they share your commitment to scientific integrity.
DOI: https://doi.org/10.37349/ec.2024.00024
Left ventricular (LV) function is typically evaluated through LV ejection fraction (EF), a robust indicator of risk, showing a nonlinear increase in mortality rates below 40%. Conversely, excessively high EF values (> 65%) also correlate with elevated mortality, following a U-shaped curve, with its nadir observed between 50% and 65%. This underscores the necessity for improved identification of the hypercontractile phenotype. However, EF is not synonymous with LV contraction function, as it can fluctuate independently of contractility due to variations in afterload, preload, heart rate, and ventricular-arterial coupling. Assessing the contractile status of the LV requires more specific metrics, such as LV elastance (or contractile force) and global longitudinal strain. Current guidelines outline various parameters for a more precise characterization of LV contractility, yet further research is warranted for validation. The true hypercontractile phenotype is evident in cardiac pathologies such as hypertrophic cardiomyopathy, ischemia with angiographically normal coronary arteries, Tako-tsubo syndrome, heart failure with preserved EF, and may also stem from systemic disorders including anemia, hyperthyroidism, liver, kidney, or pulmonary diseases. The hypercontractile phenotype constitutes a distinctive hemodynamic substrate underlying clinical manifestations such as angina, dyspnea, or arrhythmias, presenting a target for intervention through beta-blockers or specific cardiac myosin inhibitors. While EF remains pivotal for clinical classification, risk stratification, and therapeutic decision-making, integrating it with other indices of LV function can enhance the characterization of the hypercontractile phenotype.
Left ventricular (LV) function is typically evaluated through LV ejection fraction (EF), a robust indicator of risk, showing a nonlinear increase in mortality rates below 40%. Conversely, excessively high EF values (> 65%) also correlate with elevated mortality, following a U-shaped curve, with its nadir observed between 50% and 65%. This underscores the necessity for improved identification of the hypercontractile phenotype. However, EF is not synonymous with LV contraction function, as it can fluctuate independently of contractility due to variations in afterload, preload, heart rate, and ventricular-arterial coupling. Assessing the contractile status of the LV requires more specific metrics, such as LV elastance (or contractile force) and global longitudinal strain. Current guidelines outline various parameters for a more precise characterization of LV contractility, yet further research is warranted for validation. The true hypercontractile phenotype is evident in cardiac pathologies such as hypertrophic cardiomyopathy, ischemia with angiographically normal coronary arteries, Tako-tsubo syndrome, heart failure with preserved EF, and may also stem from systemic disorders including anemia, hyperthyroidism, liver, kidney, or pulmonary diseases. The hypercontractile phenotype constitutes a distinctive hemodynamic substrate underlying clinical manifestations such as angina, dyspnea, or arrhythmias, presenting a target for intervention through beta-blockers or specific cardiac myosin inhibitors. While EF remains pivotal for clinical classification, risk stratification, and therapeutic decision-making, integrating it with other indices of LV function can enhance the characterization of the hypercontractile phenotype.
DOI: https://doi.org/10.37349/ec.2024.00025
Metabolic syndrome (MetS) is known as a non-communicable disease (NCD) that affects more and more individuals. MetS is closely related to type 2 diabetes mellitus (T2DM), cardiovascular disease (CVD), obesity and inflammation. It is associated with T2DM due to the disturbance in insulin secretion/effect, eventually leading to insulin resistance (IR). The link between MetS and CVD is due to accelerated atherosclerosis in response to chronic inflammation. This literature review was based on a search in the PubMed database. All selected articles are written in English and cover a period of approximately 10 years (January 2014 to May 2023). The first selection used MeSH terms such as: “metabolic syndrome”, “type 2 diabetes mellitus”, “obesity”, “inflammation”, and “insulin resistance” and different associations between them. Titles and abstracts were analyzed. In the end, 44 articles were selected, 4 of which were meta-analysis studies. Currently, an individual is considered to have MetS if they present 3 of the following changes: increased waist circumference, increased triglycerides (TG), reduced high-density lipoprotein cholesterol (HDL-C), increased fasting blood glucose and hypertension. We believe this can often lead to a false diagnosis. The objective of this paper is to compile what we consider to be an appropriate panel of MetS indicators. The markers that stand out in this review are the lipid profile, anti- and pro-inflammatory function and oxidative stress. Considering the research, we believe that a complete panel, to correlate the most characteristic conditions of MetS, should include the following markers: TG/HDL-C ratio, small dense low-density lipoprotein cholesterol (SdLDL-C), lipid peroxidation markers, leptin/adiponectin ratio, plasminogen activator inhibitor-1 (PAI-1), activin-A and ferritin levels. Finally, it is important to expand research on the pathophysiology of MetS and confirm the most appropriate markers as well as discover new ones to correctly diagnose this condition.
Metabolic syndrome (MetS) is known as a non-communicable disease (NCD) that affects more and more individuals. MetS is closely related to type 2 diabetes mellitus (T2DM), cardiovascular disease (CVD), obesity and inflammation. It is associated with T2DM due to the disturbance in insulin secretion/effect, eventually leading to insulin resistance (IR). The link between MetS and CVD is due to accelerated atherosclerosis in response to chronic inflammation. This literature review was based on a search in the PubMed database. All selected articles are written in English and cover a period of approximately 10 years (January 2014 to May 2023). The first selection used MeSH terms such as: “metabolic syndrome”, “type 2 diabetes mellitus”, “obesity”, “inflammation”, and “insulin resistance” and different associations between them. Titles and abstracts were analyzed. In the end, 44 articles were selected, 4 of which were meta-analysis studies. Currently, an individual is considered to have MetS if they present 3 of the following changes: increased waist circumference, increased triglycerides (TG), reduced high-density lipoprotein cholesterol (HDL-C), increased fasting blood glucose and hypertension. We believe this can often lead to a false diagnosis. The objective of this paper is to compile what we consider to be an appropriate panel of MetS indicators. The markers that stand out in this review are the lipid profile, anti- and pro-inflammatory function and oxidative stress. Considering the research, we believe that a complete panel, to correlate the most characteristic conditions of MetS, should include the following markers: TG/HDL-C ratio, small dense low-density lipoprotein cholesterol (SdLDL-C), lipid peroxidation markers, leptin/adiponectin ratio, plasminogen activator inhibitor-1 (PAI-1), activin-A and ferritin levels. Finally, it is important to expand research on the pathophysiology of MetS and confirm the most appropriate markers as well as discover new ones to correctly diagnose this condition.
DOI: https://doi.org/10.37349/ec.2024.00026
This article belongs to the special issue Molecular Mechanisms of Cardiovascular Aging
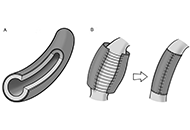
Adventitial crosslinking is a method in current investigational stage for preventing the rupture of aortic aneurysms. It is based on the photochemical crosslinking of adventitial collagen by exposure to ultraviolet A radiation. Essentially, an adventitial top layer is generated that displays enhanced mechanical properties and imparts additional strength and stiffness to the aneurysmal wall. Looking back upon the history of aortic surgery during 1940s, the aortic film wrapping, then dubbed “cellophane wrapping”, also was a procedure employed for delaying the aneurysmal rupture. In principle, the two procedures are similar in that both result in laminar composites, although the top layers differ fundamentally from each other. This review discussed in some detail the use and clinical outcomes of the aortic wrapping with artificial films, also mentioning the contemporary procedures still grouped under this umbrella term. The focus of the review was a comparative view on two procedures, the aortic film wrapping and adventitial crosslinking. It was concluded that the methods are different in many aspects, including the mechanisms of action. In fact, the promoters of adventitial crosslinking were not aware of the prior existence of aortic film wrapping. However, the achievements of the classical wrapping, by now regarded as merely historical episodes, did not discard prior knowledge, but repurposed it in a process that led to innovative strategies.
Adventitial crosslinking is a method in current investigational stage for preventing the rupture of aortic aneurysms. It is based on the photochemical crosslinking of adventitial collagen by exposure to ultraviolet A radiation. Essentially, an adventitial top layer is generated that displays enhanced mechanical properties and imparts additional strength and stiffness to the aneurysmal wall. Looking back upon the history of aortic surgery during 1940s, the aortic film wrapping, then dubbed “cellophane wrapping”, also was a procedure employed for delaying the aneurysmal rupture. In principle, the two procedures are similar in that both result in laminar composites, although the top layers differ fundamentally from each other. This review discussed in some detail the use and clinical outcomes of the aortic wrapping with artificial films, also mentioning the contemporary procedures still grouped under this umbrella term. The focus of the review was a comparative view on two procedures, the aortic film wrapping and adventitial crosslinking. It was concluded that the methods are different in many aspects, including the mechanisms of action. In fact, the promoters of adventitial crosslinking were not aware of the prior existence of aortic film wrapping. However, the achievements of the classical wrapping, by now regarded as merely historical episodes, did not discard prior knowledge, but repurposed it in a process that led to innovative strategies.
DOI: https://doi.org/10.37349/ec.2024.00027
Chagas disease is a systemic illness characterized by acute and chronic phases. If untreated, it can lead to dysfunction of vital organs, notably the heart, ultimately resulting in heart failure. Transmission primarily occurs through the feces of triatomine insects carrying the protozoan parasite Trypanosoma cruzi, either via a bite wound or intact mucous membranes. Diagnosis of Chagas disease involves serological tests, electrocardiographic findings, and imaging studies. A 58-year-old male patient from Peru with chronic dilated cardiomyopathy underwent evaluation at a tertiary care hospital. Given the uncertain etiology, a comprehensive diagnostic approach was adopted, emphasizing the pivotal role of cardiovascular magnetic resonance imaging and computed tomography angiography in managing chronic cardiomyopathy of Chagas disease. Leveraging these imaging modalities together could augment our ability to evaluate myocardial inflammation and tailor therapeutic strategies accordingly.
Chagas disease is a systemic illness characterized by acute and chronic phases. If untreated, it can lead to dysfunction of vital organs, notably the heart, ultimately resulting in heart failure. Transmission primarily occurs through the feces of triatomine insects carrying the protozoan parasite Trypanosoma cruzi, either via a bite wound or intact mucous membranes. Diagnosis of Chagas disease involves serological tests, electrocardiographic findings, and imaging studies. A 58-year-old male patient from Peru with chronic dilated cardiomyopathy underwent evaluation at a tertiary care hospital. Given the uncertain etiology, a comprehensive diagnostic approach was adopted, emphasizing the pivotal role of cardiovascular magnetic resonance imaging and computed tomography angiography in managing chronic cardiomyopathy of Chagas disease. Leveraging these imaging modalities together could augment our ability to evaluate myocardial inflammation and tailor therapeutic strategies accordingly.
DOI: https://doi.org/10.37349/ec.2024.00033
Aim:
The association of echocardiographic findings and subsequent risk of left-sided native valve endocarditis (LS-NVE) is undefined. The aim of this study was to determine if transthoracic echocardiography (TTE) measurements are associated with the subsequent development of LS-NVE in patients without cardiac predisposing conditions.
Methods:
Institutional databases were evaluated for adults diagnosed with LS-NVE from 2008 to 2020. Patients with prosthetic valves, cardiovascular implantable electronic devices, intracardiac devices, injection drug use, and predisposing cardiac conditions were excluded. Only patients who had a TTE performed 6 months to 3 years before the development of LS-NVE were included as cases. Controls were patients within the same Mayo location with a TTE report and were matched in a 1:3 ratio according to age, gender, Charlson comorbidity index, and echocardiography date.
Results:
There were 148 cases and 431 matched controls. As compared to controls, infective endocarditis (IE) cases had a higher prevalence of diabetes mellitus (46.6% vs. 30.4%) and chronic kidney disease (46.6% vs. 28.1%) (P < 0.001). Left ventricular outflow tract velocity (P = 0.017), left ventricular ejection fraction (P = 0.018), and E:e’ ratio (P = 0.050) were associated with LS-NVE.
Conclusions:
Echocardiographic measurements were associated with subsequent LS-NVE development in this pilot study. A larger cohort of LS-NVE patients, however, is needed to validate these findings.
Aim:
The association of echocardiographic findings and subsequent risk of left-sided native valve endocarditis (LS-NVE) is undefined. The aim of this study was to determine if transthoracic echocardiography (TTE) measurements are associated with the subsequent development of LS-NVE in patients without cardiac predisposing conditions.
Methods:
Institutional databases were evaluated for adults diagnosed with LS-NVE from 2008 to 2020. Patients with prosthetic valves, cardiovascular implantable electronic devices, intracardiac devices, injection drug use, and predisposing cardiac conditions were excluded. Only patients who had a TTE performed 6 months to 3 years before the development of LS-NVE were included as cases. Controls were patients within the same Mayo location with a TTE report and were matched in a 1:3 ratio according to age, gender, Charlson comorbidity index, and echocardiography date.
Results:
There were 148 cases and 431 matched controls. As compared to controls, infective endocarditis (IE) cases had a higher prevalence of diabetes mellitus (46.6% vs. 30.4%) and chronic kidney disease (46.6% vs. 28.1%) (P < 0.001). Left ventricular outflow tract velocity (P = 0.017), left ventricular ejection fraction (P = 0.018), and E:e’ ratio (P = 0.050) were associated with LS-NVE.
Conclusions:
Echocardiographic measurements were associated with subsequent LS-NVE development in this pilot study. A larger cohort of LS-NVE patients, however, is needed to validate these findings.
DOI: https://doi.org/10.37349/ec.2024.00034
