













Aim:
Breast cancer (BC) is the leading cause of female cancer-related death worldwide. The high incidence of BC has sparked interest in the viral agents role in its development. Identifying co-infection involving potential oncogenic viruses, such as human papillomavirus (HPV), Epstein-Barr virus (EBV), mouse mammary tumor virus (MMTV), and Simian virus 40 (SV40), may improve early detection and treatment strategies of BC. However, the involvement of these viral co-infections in invasive breast cancer (IBC) has not been elucidated.
Methods:
To investigate this eventual co-infection, screening of viral DNAs isolated from 120 fresh IBC tissue biopsies was performed using a polymerase chain reaction. Statistical analysis were conducted to assess the correlation between viral prevalence and IBC clinicopathological features.
Results:
Our findings revealed the prevalence of EBV (67.1%), HPV (45.7%), MMTV (72.9%), and SV40 (22.9%) in IBC samples. Co-infection rates were as follows: EBV/HPV (17.14%), EBV/MMTV (22.86%), EBV/SV40 (4.28%), and HPV/MMTV (11.43%). Triple infection with EBV, HPV, and MMTV was observed in 5.71% of cases. Statistically significant associations were identified between: EBV and histological grade, tumour size and stage, and progesterone receptor (PR) and estrogen receptor (ER) status; HPV and histological grade, tumour stage, and PR status; MMTV and histological type, as well as PR and ER status; and SV40 and histological grade and PR status.
Conclusions:
Although the prevalence of HPV, EBV, MMTV, and SV40 coinfection in Moroccan IBC patients is low, their potential synergistic role in breast carcinogenesis needs to be further investigated, in order to identify new etiological factors for BC.
Aim:
Breast cancer (BC) is the leading cause of female cancer-related death worldwide. The high incidence of BC has sparked interest in the viral agents role in its development. Identifying co-infection involving potential oncogenic viruses, such as human papillomavirus (HPV), Epstein-Barr virus (EBV), mouse mammary tumor virus (MMTV), and Simian virus 40 (SV40), may improve early detection and treatment strategies of BC. However, the involvement of these viral co-infections in invasive breast cancer (IBC) has not been elucidated.
Methods:
To investigate this eventual co-infection, screening of viral DNAs isolated from 120 fresh IBC tissue biopsies was performed using a polymerase chain reaction. Statistical analysis were conducted to assess the correlation between viral prevalence and IBC clinicopathological features.
Results:
Our findings revealed the prevalence of EBV (67.1%), HPV (45.7%), MMTV (72.9%), and SV40 (22.9%) in IBC samples. Co-infection rates were as follows: EBV/HPV (17.14%), EBV/MMTV (22.86%), EBV/SV40 (4.28%), and HPV/MMTV (11.43%). Triple infection with EBV, HPV, and MMTV was observed in 5.71% of cases. Statistically significant associations were identified between: EBV and histological grade, tumour size and stage, and progesterone receptor (PR) and estrogen receptor (ER) status; HPV and histological grade, tumour stage, and PR status; MMTV and histological type, as well as PR and ER status; and SV40 and histological grade and PR status.
Conclusions:
Although the prevalence of HPV, EBV, MMTV, and SV40 coinfection in Moroccan IBC patients is low, their potential synergistic role in breast carcinogenesis needs to be further investigated, in order to identify new etiological factors for BC.
DOI: https://doi.org/10.37349/emed.2025.1001304
This article belongs to the special issue Breast Cancer: Basic and Clinical Advances
Aim:
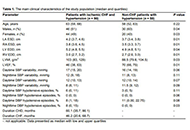
Although the prevalence of coronary heart disease (CHD) and hypertension which are the most common causes of the development and progression of chronic heart failure (CHF) is high, 24-hour ambulatory blood pressure (BP) monitoring (ABPM) in patients with CHF is not mandatory to be performed. The growing number of evidence suggests that excessive decrease in BP which clearly reflects increased BP variability (BPV) affects the survival of patients with heart failure (HF). The objective of the study was to investigate the relationship between the parameters specific to CHF severity and features of daily BP profiles in patients with ischemic CHF and hypertension.
Methods:
Ninety patients with functional class II–IV of CHF and CHD (the main group) and 50 non-CHF patients with hypertension (the comparative group) were examined. The transthoracic echocardiography (TTE) [atrial end-systolic dimension (ESD), ventricular end-diastolic dimension (EDD), left ventricular mass index (LVMI), and left ventricular ejection fraction (LVEF)] and 24-hour ABPM (BPV parameters and proportions of hypotensive episodes) were performed. The relationships between the abovementioned parameters were evaluated using the univariate correlation analysis and stepwise multiple linear regression.
Results:
Higher functional class of CHF is found to be associated with a higher incidence of daytime systolic BP (SBP) decline and nighttime SBP and diastolic BP (DBP) variability while higher LVEF is related to the hypotensive episodes regardless of CHF.
Conclusions:
It appears that the larger trials involving CHF patients with reduced LVEF should be conducted to clarify the obtained results.
Aim:
Although the prevalence of coronary heart disease (CHD) and hypertension which are the most common causes of the development and progression of chronic heart failure (CHF) is high, 24-hour ambulatory blood pressure (BP) monitoring (ABPM) in patients with CHF is not mandatory to be performed. The growing number of evidence suggests that excessive decrease in BP which clearly reflects increased BP variability (BPV) affects the survival of patients with heart failure (HF). The objective of the study was to investigate the relationship between the parameters specific to CHF severity and features of daily BP profiles in patients with ischemic CHF and hypertension.
Methods:
Ninety patients with functional class II–IV of CHF and CHD (the main group) and 50 non-CHF patients with hypertension (the comparative group) were examined. The transthoracic echocardiography (TTE) [atrial end-systolic dimension (ESD), ventricular end-diastolic dimension (EDD), left ventricular mass index (LVMI), and left ventricular ejection fraction (LVEF)] and 24-hour ABPM (BPV parameters and proportions of hypotensive episodes) were performed. The relationships between the abovementioned parameters were evaluated using the univariate correlation analysis and stepwise multiple linear regression.
Results:
Higher functional class of CHF is found to be associated with a higher incidence of daytime systolic BP (SBP) decline and nighttime SBP and diastolic BP (DBP) variability while higher LVEF is related to the hypotensive episodes regardless of CHF.
Conclusions:
It appears that the larger trials involving CHF patients with reduced LVEF should be conducted to clarify the obtained results.
DOI: https://doi.org/10.37349/emed.2024.00209
Aim:
Cigarette smoking is an addictive behavior that requires high motivation to change, a phenotype related to the functional activity of the brain. The study aims to examine motivation to change among cigarette smokers and to study the association between functional brain activity and motivation to change smoking behaviors.
Methods:
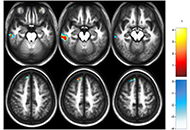
Motivation to change smoking behaviors of 107 current smokers receiving services in a university hospital was obtained using the Stages of Change Readiness and Treatment Eagerness Scale (SOCRATES). Brain activities related to motivation to change were also explored in a subgroup using functional magnetic resonance imaging (fMRI).
Results:
The results showed that most of the current smokers (n = 68, 63.6%) were low motivated to change despite receiving health-related services. Brain activities in the left of the temporal, frontal gyrus, and superior medial gyrus of smokers with motivation were greater activated than those without. In contrast, the brain activities in the left precentral gyrus and bilateral paracentral lobules of smokers without motivation were greater activated.
Conclusions:
These preliminary results show the differences in brain activities between smokers with and without motivation to change and warrant further research to see if motivated smokers can quit smoking using a series of strategies based on their functional activities of the brain.
Aim:
Cigarette smoking is an addictive behavior that requires high motivation to change, a phenotype related to the functional activity of the brain. The study aims to examine motivation to change among cigarette smokers and to study the association between functional brain activity and motivation to change smoking behaviors.
Methods:
Motivation to change smoking behaviors of 107 current smokers receiving services in a university hospital was obtained using the Stages of Change Readiness and Treatment Eagerness Scale (SOCRATES). Brain activities related to motivation to change were also explored in a subgroup using functional magnetic resonance imaging (fMRI).
Results:
The results showed that most of the current smokers (n = 68, 63.6%) were low motivated to change despite receiving health-related services. Brain activities in the left of the temporal, frontal gyrus, and superior medial gyrus of smokers with motivation were greater activated than those without. In contrast, the brain activities in the left precentral gyrus and bilateral paracentral lobules of smokers without motivation were greater activated.
Conclusions:
These preliminary results show the differences in brain activities between smokers with and without motivation to change and warrant further research to see if motivated smokers can quit smoking using a series of strategies based on their functional activities of the brain.
DOI: https://doi.org/10.37349/emed.2023.00154
This article belongs to the special issue The Biological Basis of Substance Use Disorders
The idea that proteins are the main determining factors in the functioning of cells and organisms, and their dysfunctions are the first cause of pathologies, has been predominant in biology and biomedicine until recently. This protein-centered view was too simplistic and failed to explain the physiological and pathological complexity of the cell. About 80% of the human genome is dynamically and pervasively transcribed, mostly as non-protein-coding RNAs (ncRNAs), which competitively interact with each other and with coding RNAs generating a complex RNA network regulating RNA processing, stability, and translation and, accordingly, fine-tuning the gene expression of the cells. Qualitative and quantitative dysregulations of RNA-RNA interaction networks are strongly involved in the onset and progression of many pathologies, including cancers and degenerative diseases. This review will summarize the RNA species involved in the competitive endogenous RNA network, their mechanisms of action, and involvement in pathological phenotypes. Moreover, it will give an overview of the most advanced experimental and computational methods to dissect and rebuild RNA networks.
The idea that proteins are the main determining factors in the functioning of cells and organisms, and their dysfunctions are the first cause of pathologies, has been predominant in biology and biomedicine until recently. This protein-centered view was too simplistic and failed to explain the physiological and pathological complexity of the cell. About 80% of the human genome is dynamically and pervasively transcribed, mostly as non-protein-coding RNAs (ncRNAs), which competitively interact with each other and with coding RNAs generating a complex RNA network regulating RNA processing, stability, and translation and, accordingly, fine-tuning the gene expression of the cells. Qualitative and quantitative dysregulations of RNA-RNA interaction networks are strongly involved in the onset and progression of many pathologies, including cancers and degenerative diseases. This review will summarize the RNA species involved in the competitive endogenous RNA network, their mechanisms of action, and involvement in pathological phenotypes. Moreover, it will give an overview of the most advanced experimental and computational methods to dissect and rebuild RNA networks.
DOI: https://doi.org/10.37349/emed.2023.00159
This article belongs to the special issue RNA World in Health and Disease
Abnormal energy metabolism is one of the ten hallmarks of tumors, and tumor cell metabolism provides energy and a suitable microenvironment for tumorigenesis and metastasis. Tumor cells can consume large amounts of glucose and produce large amounts of lactate through glycolysis even in the presence of oxygen, a process called aerobic glycolysis, also known as the Warburg effect. Lactate is the end product of the aerobic glycolysis. Lactate dehydrogenase A (LDHA), which is highly expressed in cancer cells, promotes lactate production and transports lactate to the tumor microenvironment and is taken up by surrounding stromal cells under the action of monocarboxylate transporter 1/4 (MCT1/4), which in turn influences the immune response and enhances the invasion and metastasis of cancer cells. Therapeutic strategies targeting lactate metabolism have been intensively investigated, focusing on its metastasis-promoting properties and various target inhibitors; AZD3965, an MCT1 inhibitor, has entered phase I clinical trials, and the LDHA inhibitor N-hydroxyindole (NHI) has shown cancer therapeutic activity in pre-clinical studies. Interventions targeting lactate metabolism are emerging as a promising option for cancer therapy, with chemotherapy or radiotherapy combined with lactate-metabolism-targeted drugs adding to the effectiveness of cancer treatment. Based on current research, this article outlines the role of lactate metabolism in tumor metastasis and the potential value of inhibitors targeting lactate metabolism in cancer therapy.
Abnormal energy metabolism is one of the ten hallmarks of tumors, and tumor cell metabolism provides energy and a suitable microenvironment for tumorigenesis and metastasis. Tumor cells can consume large amounts of glucose and produce large amounts of lactate through glycolysis even in the presence of oxygen, a process called aerobic glycolysis, also known as the Warburg effect. Lactate is the end product of the aerobic glycolysis. Lactate dehydrogenase A (LDHA), which is highly expressed in cancer cells, promotes lactate production and transports lactate to the tumor microenvironment and is taken up by surrounding stromal cells under the action of monocarboxylate transporter 1/4 (MCT1/4), which in turn influences the immune response and enhances the invasion and metastasis of cancer cells. Therapeutic strategies targeting lactate metabolism have been intensively investigated, focusing on its metastasis-promoting properties and various target inhibitors; AZD3965, an MCT1 inhibitor, has entered phase I clinical trials, and the LDHA inhibitor N-hydroxyindole (NHI) has shown cancer therapeutic activity in pre-clinical studies. Interventions targeting lactate metabolism are emerging as a promising option for cancer therapy, with chemotherapy or radiotherapy combined with lactate-metabolism-targeted drugs adding to the effectiveness of cancer treatment. Based on current research, this article outlines the role of lactate metabolism in tumor metastasis and the potential value of inhibitors targeting lactate metabolism in cancer therapy.
DOI: https://doi.org/10.37349/emed.2023.00160
Aim:
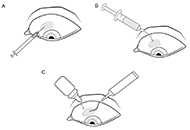
The use of 5-fluorouracil in glaucoma surgery is associated with a high risk of corneal complications, as even minimal doses of the drug at the ocular surface inhibit corneal epithelial cell division and lead to corneal epitheliopathy and erosion. The aim of this study was to evaluate the clinical and functional results of the proposed method of postoperative adjuvant subconjunctival injection of 5-fluorouracil after non-penetrating deep sclerectomy (NPDS) in comparison with the control group.
Methods:
Patients with primary open-angle glaucoma who underwent NPDS and received at least 1 subconjunctival injection of 5-fluorouracil in the postoperative period were included in a two-group retrospective comparative study. Patients who received a subconjunctival injection of 5-fluorouracil after surgery using the standard technique were included in Group 1; Group 2 included patients who received an injection using the proposed method. Best-corrected visual acuity (BCVA), intraocular pressure (IOP), rate of corneal complications, and number of office visits during the first 4 weeks after surgery were analysed.
Results:
The compared groups did not differ in demographic characteristics, preoperative BCVA, and IOP parameters. Fluorescein-stained corneal epithelial defects were statistically significantly more frequent in Group 1 compared to Group 2, P < 0.001. Four weeks post NPDS IOP reduction was greater in Group 2, P = 0.042. Mean BCVA loss was 1.9 lines in Group 1 and 1.3 lines in Group 2, P < 0.001. The number of follow-up visits during the first month after surgery was lower in Group 2 than in Group 1, P = 0.002.
Conclusions:
The proposed method was simple and effective in reducing the risk of corneal epithelial defects after subconjunctival injection of 5-fluorouracil, significantly improving clinical and functional outcomes of NPDS and reducing the need for outpatient visits.
Aim:
The use of 5-fluorouracil in glaucoma surgery is associated with a high risk of corneal complications, as even minimal doses of the drug at the ocular surface inhibit corneal epithelial cell division and lead to corneal epitheliopathy and erosion. The aim of this study was to evaluate the clinical and functional results of the proposed method of postoperative adjuvant subconjunctival injection of 5-fluorouracil after non-penetrating deep sclerectomy (NPDS) in comparison with the control group.
Methods:
Patients with primary open-angle glaucoma who underwent NPDS and received at least 1 subconjunctival injection of 5-fluorouracil in the postoperative period were included in a two-group retrospective comparative study. Patients who received a subconjunctival injection of 5-fluorouracil after surgery using the standard technique were included in Group 1; Group 2 included patients who received an injection using the proposed method. Best-corrected visual acuity (BCVA), intraocular pressure (IOP), rate of corneal complications, and number of office visits during the first 4 weeks after surgery were analysed.
Results:
The compared groups did not differ in demographic characteristics, preoperative BCVA, and IOP parameters. Fluorescein-stained corneal epithelial defects were statistically significantly more frequent in Group 1 compared to Group 2, P < 0.001. Four weeks post NPDS IOP reduction was greater in Group 2, P = 0.042. Mean BCVA loss was 1.9 lines in Group 1 and 1.3 lines in Group 2, P < 0.001. The number of follow-up visits during the first month after surgery was lower in Group 2 than in Group 1, P = 0.002.
Conclusions:
The proposed method was simple and effective in reducing the risk of corneal epithelial defects after subconjunctival injection of 5-fluorouracil, significantly improving clinical and functional outcomes of NPDS and reducing the need for outpatient visits.
DOI: https://doi.org/10.37349/emed.2023.00155
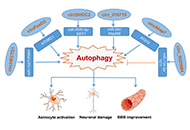
Stroke, a central nervous system (CNS) injury, is responsible for the second leading cause of death in the world, bringing a great burden on the world. Stroke is normally divided into ischemic and hemorrhagic stroke, among which ischemic stroke takes up 87% proportion. Accumulating evidence has denoted a rather pivotal role for autophagy in the pathogenesis of ischemic stroke, which is activated in neuronal cells, glial cells, and endothelial cells. Besides, circular RNAs (circRNAs), a novel type of epigenetic regulation, are highly expressed in the CNS and are involved in the process of CNS diseases, which is regarded as an important molecular mechanism in ischemic stroke. Meanwhile, circRNA and autophagy have a significant correlation. The intracellular signaling pathways regulating autophagy can either restrain or activate autophagy. However, under the circumstances of ischemic stroke, the precise communication between circRNA and stroke is largely unknown. This review aims to provide a summary of the relationship between circRNA, autophagy, and ischemic stroke, as well as the current research advancements in understanding how circRNA regulates autophagy in the context of stroke.
Stroke, a central nervous system (CNS) injury, is responsible for the second leading cause of death in the world, bringing a great burden on the world. Stroke is normally divided into ischemic and hemorrhagic stroke, among which ischemic stroke takes up 87% proportion. Accumulating evidence has denoted a rather pivotal role for autophagy in the pathogenesis of ischemic stroke, which is activated in neuronal cells, glial cells, and endothelial cells. Besides, circular RNAs (circRNAs), a novel type of epigenetic regulation, are highly expressed in the CNS and are involved in the process of CNS diseases, which is regarded as an important molecular mechanism in ischemic stroke. Meanwhile, circRNA and autophagy have a significant correlation. The intracellular signaling pathways regulating autophagy can either restrain or activate autophagy. However, under the circumstances of ischemic stroke, the precise communication between circRNA and stroke is largely unknown. This review aims to provide a summary of the relationship between circRNA, autophagy, and ischemic stroke, as well as the current research advancements in understanding how circRNA regulates autophagy in the context of stroke.
DOI: https://doi.org/10.37349/emed.2023.00157
Broncho-alveolar lavage (BAL) represents a safe tool for the differential diagnosis of various pulmonary fibrotic diseases. Idiopathic pulmonary fibrosis (IPF) belongs to a heterogeneous group of diseases, interstitial lung disease (ILD), presenting a progressive impairment of pulmonary functions. IPF is characterized by the excessive accumulation of extracellular matrix (ECM) in the alveolar parenchyma that may lead to irreversible pulmonary remodeling. Although the exact pathogenetic mechanisms leading to IPF development are still unclear it has been demonstrated that fibroblasts differentiating toward myofibroblasts are the major actors involved in this process. The possibility of obtaining and expanding fibroblasts from the BAL of ILD patients for research purposes has been recently explored. This approach is discussed here as a reliable chance, helpful to advance the scientific community knowledge and to devise two- and three-dimensional (2D/3D) pre-clinical in vitro models of these diseases, further overcoming technical and ethical concerns related to the use of fibroblasts derived from tissue biopsy.
Broncho-alveolar lavage (BAL) represents a safe tool for the differential diagnosis of various pulmonary fibrotic diseases. Idiopathic pulmonary fibrosis (IPF) belongs to a heterogeneous group of diseases, interstitial lung disease (ILD), presenting a progressive impairment of pulmonary functions. IPF is characterized by the excessive accumulation of extracellular matrix (ECM) in the alveolar parenchyma that may lead to irreversible pulmonary remodeling. Although the exact pathogenetic mechanisms leading to IPF development are still unclear it has been demonstrated that fibroblasts differentiating toward myofibroblasts are the major actors involved in this process. The possibility of obtaining and expanding fibroblasts from the BAL of ILD patients for research purposes has been recently explored. This approach is discussed here as a reliable chance, helpful to advance the scientific community knowledge and to devise two- and three-dimensional (2D/3D) pre-clinical in vitro models of these diseases, further overcoming technical and ethical concerns related to the use of fibroblasts derived from tissue biopsy.
DOI: https://doi.org/10.37349/emed.2023.00156
This article belongs to the special issue Lung Fibrosis—Models and Mechanisms
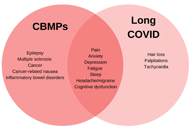
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection can result in a range of persistent symptoms impacting everyday functioning for a considerable proportion of patients, a condition termed Long coronavirus disease (COVID) or post COVID-19 syndrome. The severity and set of symptoms vary between patients, and include fatigue, cognitive dysfunction, sleep disturbances, palpitations, tachycardia, pain, depression, and anxiety. The high prevalence of Long COVID combined with the lack of treatment approaches has resulted in considerable unmet clinical needs. There is a growing body of evidence that cannabis-based medicinal products (CBMPs) can be used to treat symptoms including pain, anxiety, depression, fatigue, sleep, headaches, and cognitive dysfunction, which are commonly reported in Long COVID. This article provides an overview of the pathophysiology of Long COVID and discusses preliminary pre-clinical, clinical trials, and real-world evidence (RWE) for CBMPs in the context of Long COVID. This review summarises current clinical trials and studies exploring CBMPs in Long COVID. The current evidence provides a rationale to further explore CBMPs as a treatment for Long COVID symptoms. In addition to further randomised controlled trials (RCTs), the increasing availability of CBMPs globally, coupled with the continued prevalence of Long COVID in the population, also highlights the value of real-world data in the research of CBMPs in Long COVID. Critically, there is an evident need for multidisciplinary approaches of CBMPs and Long COVID in real-world clinical practice settings.
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection can result in a range of persistent symptoms impacting everyday functioning for a considerable proportion of patients, a condition termed Long coronavirus disease (COVID) or post COVID-19 syndrome. The severity and set of symptoms vary between patients, and include fatigue, cognitive dysfunction, sleep disturbances, palpitations, tachycardia, pain, depression, and anxiety. The high prevalence of Long COVID combined with the lack of treatment approaches has resulted in considerable unmet clinical needs. There is a growing body of evidence that cannabis-based medicinal products (CBMPs) can be used to treat symptoms including pain, anxiety, depression, fatigue, sleep, headaches, and cognitive dysfunction, which are commonly reported in Long COVID. This article provides an overview of the pathophysiology of Long COVID and discusses preliminary pre-clinical, clinical trials, and real-world evidence (RWE) for CBMPs in the context of Long COVID. This review summarises current clinical trials and studies exploring CBMPs in Long COVID. The current evidence provides a rationale to further explore CBMPs as a treatment for Long COVID symptoms. In addition to further randomised controlled trials (RCTs), the increasing availability of CBMPs globally, coupled with the continued prevalence of Long COVID in the population, also highlights the value of real-world data in the research of CBMPs in Long COVID. Critically, there is an evident need for multidisciplinary approaches of CBMPs and Long COVID in real-world clinical practice settings.
DOI: https://doi.org/10.37349/emed.2023.00158
This article belongs to the special issue Beyond Weed: Clinical Applications of Cannabis and Cannabinoids
The development of patient-specific prosthetics, medication administration, the manufacture of tissues and organs, and surgical planning have all benefited significantly from the use of three-dimensional (3D) printing during the past few decades. The enthusiasm for customized healthcare has increased because the United States of America launched its Precision Medicine Initiative in 2015. In a nutshell, the phrase “personalized medicine” refers to medical care that is tailored to the patient. Nevertheless, the biomedical materials utilized in 3D printing are often stable and can’t react or be adaptive and intelligent in the body’s interior environment. Ex-situ fabrication of these substances, which includes printing on a flat substrate before releasing it onto the target surface, may cause a discrepancy between the printed portion and the target areas. The 3D printing is one method that might be used to provide customized treatment. The four-dimensional (4D) printing is developed while employing components that can be tweaked with stimulation. Several researchers have been looking at a new area recently that blends medicines with 3D and 4D printing. The development of 4D printing overcomes a number of these issues and creates a promising future for the biomedical industry. Smart materials that have been pre-programmed can be used in 4D printing to create structures that react interactively to outside stimuli. Despite these benefits, dynamic materials created using 4D technology remain in their development. As a result, several ideas for pharmaceutical products and formulas that may be customized and printed have emerged. Furthermore, Spritam®, the first medicine produced by 3D printing, has indeed reached a medical facility. This paper offers a summary of several 3D and 4D printing technologies and how they are used in the pharmaceutical industry for customized medicine and drug delivery systems.
The development of patient-specific prosthetics, medication administration, the manufacture of tissues and organs, and surgical planning have all benefited significantly from the use of three-dimensional (3D) printing during the past few decades. The enthusiasm for customized healthcare has increased because the United States of America launched its Precision Medicine Initiative in 2015. In a nutshell, the phrase “personalized medicine” refers to medical care that is tailored to the patient. Nevertheless, the biomedical materials utilized in 3D printing are often stable and can’t react or be adaptive and intelligent in the body’s interior environment. Ex-situ fabrication of these substances, which includes printing on a flat substrate before releasing it onto the target surface, may cause a discrepancy between the printed portion and the target areas. The 3D printing is one method that might be used to provide customized treatment. The four-dimensional (4D) printing is developed while employing components that can be tweaked with stimulation. Several researchers have been looking at a new area recently that blends medicines with 3D and 4D printing. The development of 4D printing overcomes a number of these issues and creates a promising future for the biomedical industry. Smart materials that have been pre-programmed can be used in 4D printing to create structures that react interactively to outside stimuli. Despite these benefits, dynamic materials created using 4D technology remain in their development. As a result, several ideas for pharmaceutical products and formulas that may be customized and printed have emerged. Furthermore, Spritam®, the first medicine produced by 3D printing, has indeed reached a medical facility. This paper offers a summary of several 3D and 4D printing technologies and how they are used in the pharmaceutical industry for customized medicine and drug delivery systems.
DOI: https://doi.org/10.37349/emed.2023.00161
This article belongs to the special issue Exploration of 3D and 4D Printing in the Biomedical and Personalized Medicine Fields: Merits and Challenges
The current literature findings on autophagy’s beneficial and detrimental roles in diabetes mellitus (DM) and diabetes-related comorbidities were reviewed. The effects of oral hypoglycaemic medicines and autophagy in DM. Autophagy plays an important function in cellular homeostasis by promoting cell survival or initiating cell death in physiological settings was also assessed. Although autophagy protects insulin-target tissues, organelle failure caused by autophagy malfunction influences DM and other metabolic diseases. Endoplasmic reticulum and oxidative stress enhance autophagy levels, making it easier to regulate stress-induced intracellular changes. Evidence suggests that autophagy-caused cell death can occur when autophagy is overstimulated and constitutively activated, which might prevent or develop DM. Even though the precise role of autophagy in DM complications is uncertain, deregulation of the autophagic machinery is strongly linked to beta cell destruction and the aetiology of DM. Thus, improving autophagy dysfunction is a possible therapeutic objective in treating DM and other metabolic disorders.
The current literature findings on autophagy’s beneficial and detrimental roles in diabetes mellitus (DM) and diabetes-related comorbidities were reviewed. The effects of oral hypoglycaemic medicines and autophagy in DM. Autophagy plays an important function in cellular homeostasis by promoting cell survival or initiating cell death in physiological settings was also assessed. Although autophagy protects insulin-target tissues, organelle failure caused by autophagy malfunction influences DM and other metabolic diseases. Endoplasmic reticulum and oxidative stress enhance autophagy levels, making it easier to regulate stress-induced intracellular changes. Evidence suggests that autophagy-caused cell death can occur when autophagy is overstimulated and constitutively activated, which might prevent or develop DM. Even though the precise role of autophagy in DM complications is uncertain, deregulation of the autophagic machinery is strongly linked to beta cell destruction and the aetiology of DM. Thus, improving autophagy dysfunction is a possible therapeutic objective in treating DM and other metabolic disorders.
DOI: https://doi.org/10.37349/emed.2023.00162
Wound healing is a very dynamic and complex process as it involves the patient, wound-level parameters, as well as biological, environmental, and socioeconomic factors. Its process includes hemostasis, inflammation, proliferation, and remodeling. Evaluation of wound components such as angiogenesis, inflammation, restoration of connective tissue matrix, wound contraction, remodeling, and re-epithelization would detail the healing process. Understanding key mechanisms in the healing process is critical to wound research. Elucidating its healing complexity would enable control and optimize the processes for achieving faster healing, preventing wound complications, and undesired outcomes such as infection, periwound dermatitis and edema, hematomas, dehiscence, maceration, or scarring. Wound assessment is an essential step for selecting an appropriate treatment and evaluating the wound healing process. The use of artificial intelligence (AI) as advanced computer-assisted methods is promising for gaining insights into wound assessment and healing. As AI-based approaches have been explored for various applications in wound care and research, this paper provides an overview of recent studies exploring the application of AI and its technical developments and suitability for accurate wound assessment and prediction of wound healing. Several studies have been done across the globe, especially in North America, Europe, Oceania, and Asia. The results of these studies have shown that AI-based approaches are promising for wound assessment and prediction of wound healing. However, there are still some limitations and challenges that need to be addressed. This paper also discusses the challenges and limitations of AI-based approaches for wound assessment and prediction of wound healing. The paper concludes with a discussion of future research directions and recommendations for the use of AI-based approaches for wound assessment and prediction of wound healing.
Wound healing is a very dynamic and complex process as it involves the patient, wound-level parameters, as well as biological, environmental, and socioeconomic factors. Its process includes hemostasis, inflammation, proliferation, and remodeling. Evaluation of wound components such as angiogenesis, inflammation, restoration of connective tissue matrix, wound contraction, remodeling, and re-epithelization would detail the healing process. Understanding key mechanisms in the healing process is critical to wound research. Elucidating its healing complexity would enable control and optimize the processes for achieving faster healing, preventing wound complications, and undesired outcomes such as infection, periwound dermatitis and edema, hematomas, dehiscence, maceration, or scarring. Wound assessment is an essential step for selecting an appropriate treatment and evaluating the wound healing process. The use of artificial intelligence (AI) as advanced computer-assisted methods is promising for gaining insights into wound assessment and healing. As AI-based approaches have been explored for various applications in wound care and research, this paper provides an overview of recent studies exploring the application of AI and its technical developments and suitability for accurate wound assessment and prediction of wound healing. Several studies have been done across the globe, especially in North America, Europe, Oceania, and Asia. The results of these studies have shown that AI-based approaches are promising for wound assessment and prediction of wound healing. However, there are still some limitations and challenges that need to be addressed. This paper also discusses the challenges and limitations of AI-based approaches for wound assessment and prediction of wound healing. The paper concludes with a discussion of future research directions and recommendations for the use of AI-based approaches for wound assessment and prediction of wound healing.
DOI: https://doi.org/10.37349/emed.2023.00163
Aim:
Childhood obesity is a global health concern that affects the daily life of children. It has a complex pathogenesis that involves genetic and nutritional factors among others. Moreover, the dysbiosis of gut microbiota has been recently associated with the development and progression of obesity.
Methods:
A total of 43 faecal samples were collected from Saudi children; among them, 26 were normal and 17 were obese. Whole genomic DNA was extracted from their faecal samples and sequenced using an Illumina Sequencing platform.
Results:
The gut microbiota was dominated by Phyla Firmicutes (69.00%) and Bacteroidetes (20.00%), followed by Actinobacteria (8.50%). In children with obesity, the abundance of Firmicutes was decreased, while Bacteroidetes was relatively enriched. Verrucomicrobia and Proteobacteria were not detected in the obese group, but they were found in low abundance in the control group. Phylum Firmicutes was dominated by the families Ruminococcaceae (17.86%) and Lachnospiraceae (41.20%). Less Ruminococcaceae was found in the obese group. Phylum Bacteroidetes was dominated by families Bacteroidaceae (12.98%) and Prevotellaceae (4.10%), which were enriched in the obese group. Genus Blautia (14.29%) was highly abundant, followed by Bacteroides (12.98%), Faecalibacterium (10.08%), Bifidobacterium (7.96%), and Prevotella (5.04%). Ruminococcus_g2 and _g4, Subdoligranulum, Roseburia, Fusicatenibacter, Anaerostipes, and Faecalibacterium were decreased (P > 0.05) in the obese group, while Streptococcus, Agathobacter, Prevotella, Bacteroides, and Bifidobacterium were increased (P > 0.05).
Conclusions:
In conclusion, a diverse bacterial community was profiled in Saudi preschool children, and changes in bacterial community composition were observed between obese- and normal-weight children.
Aim:
Childhood obesity is a global health concern that affects the daily life of children. It has a complex pathogenesis that involves genetic and nutritional factors among others. Moreover, the dysbiosis of gut microbiota has been recently associated with the development and progression of obesity.
Methods:
A total of 43 faecal samples were collected from Saudi children; among them, 26 were normal and 17 were obese. Whole genomic DNA was extracted from their faecal samples and sequenced using an Illumina Sequencing platform.
Results:
The gut microbiota was dominated by Phyla Firmicutes (69.00%) and Bacteroidetes (20.00%), followed by Actinobacteria (8.50%). In children with obesity, the abundance of Firmicutes was decreased, while Bacteroidetes was relatively enriched. Verrucomicrobia and Proteobacteria were not detected in the obese group, but they were found in low abundance in the control group. Phylum Firmicutes was dominated by the families Ruminococcaceae (17.86%) and Lachnospiraceae (41.20%). Less Ruminococcaceae was found in the obese group. Phylum Bacteroidetes was dominated by families Bacteroidaceae (12.98%) and Prevotellaceae (4.10%), which were enriched in the obese group. Genus Blautia (14.29%) was highly abundant, followed by Bacteroides (12.98%), Faecalibacterium (10.08%), Bifidobacterium (7.96%), and Prevotella (5.04%). Ruminococcus_g2 and _g4, Subdoligranulum, Roseburia, Fusicatenibacter, Anaerostipes, and Faecalibacterium were decreased (P > 0.05) in the obese group, while Streptococcus, Agathobacter, Prevotella, Bacteroides, and Bifidobacterium were increased (P > 0.05).
Conclusions:
In conclusion, a diverse bacterial community was profiled in Saudi preschool children, and changes in bacterial community composition were observed between obese- and normal-weight children.
DOI: https://doi.org/10.37349/emed.2023.00164
This article belongs to the special issue The Role of Gut Microbiota and its Metabolites in Gastrointestinal Diseases
Aim:
The purpose of this study was to examine the association among body mass, blood pressure (BP), and cognitive functioning for octogenarians and centenarians.
Methods:
A total of 300 participants (221 centenarians and 79 octogenarians) from the Georgia Centenarian Study were included in this study. Demographic variables included age, gender, and ethnicity. Body mass was measured with the body mass index (BMI), and systolic and diastolic BP, as well as mean arterial pressure (MAP) and the Mini-Mental Status Examination (MMSE) were assessed.
Results:
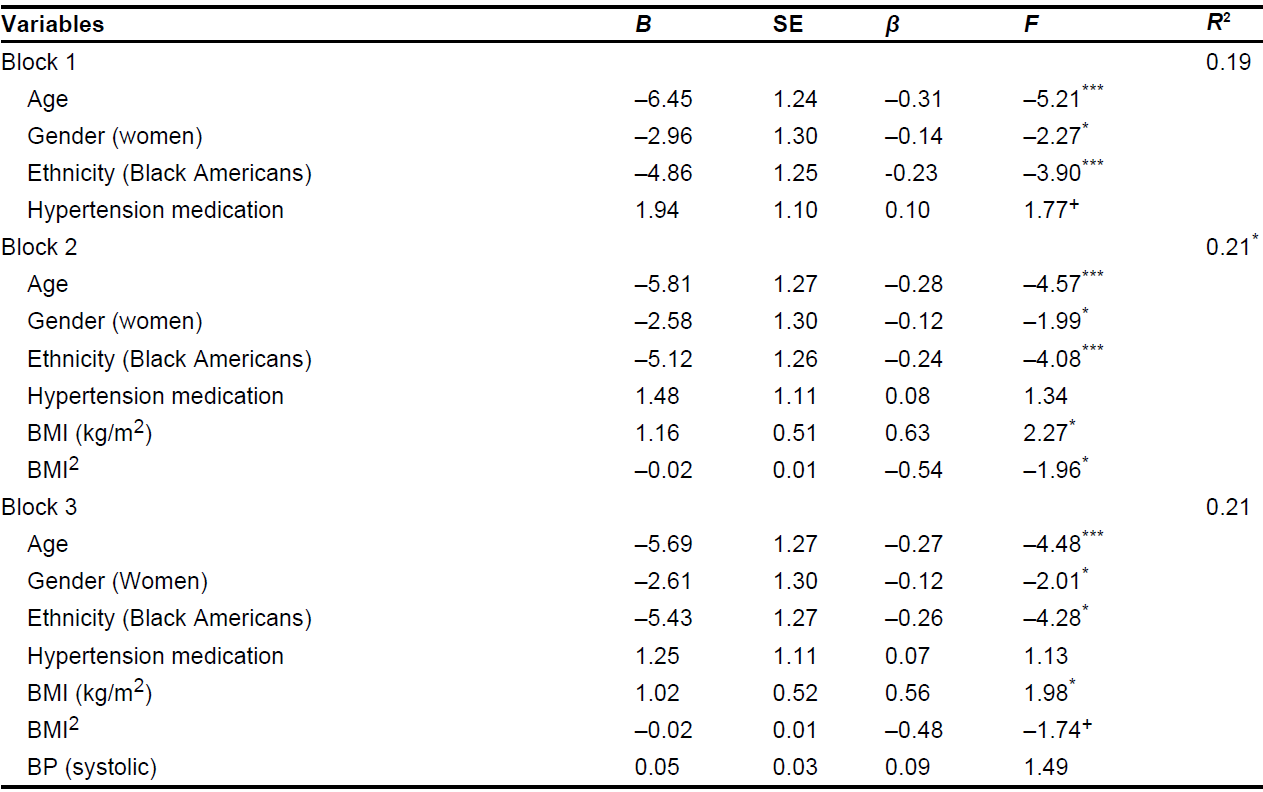
Results showed age differences indicating that centenarians had lower BMI and MMSE scores when compared to octogenarians. Women had lower cognitive functioning scores compared to men. Black Americans had higher BMI and BP as well as lower MMSE scores. Participants with low BMI values (< 18.5 kg/m2) and normal BP had a significantly lower MMSE score when compared to those with elevated BMI values (≥ 25 kg/m2 to < 30 kg/m2) and high BP. Multiple regression analyses determined that age, gender, ethnicity, and BMI were significantly associated with cognitive function in very late life.
Conclusions:
The results suggest that extreme values of body mass (low and high) in combination with normal BP (< 130 mmHg) are potential risk factors for compromised cognition.
Aim:
The purpose of this study was to examine the association among body mass, blood pressure (BP), and cognitive functioning for octogenarians and centenarians.
Methods:
A total of 300 participants (221 centenarians and 79 octogenarians) from the Georgia Centenarian Study were included in this study. Demographic variables included age, gender, and ethnicity. Body mass was measured with the body mass index (BMI), and systolic and diastolic BP, as well as mean arterial pressure (MAP) and the Mini-Mental Status Examination (MMSE) were assessed.
Results:
Results showed age differences indicating that centenarians had lower BMI and MMSE scores when compared to octogenarians. Women had lower cognitive functioning scores compared to men. Black Americans had higher BMI and BP as well as lower MMSE scores. Participants with low BMI values (< 18.5 kg/m2) and normal BP had a significantly lower MMSE score when compared to those with elevated BMI values (≥ 25 kg/m2 to < 30 kg/m2) and high BP. Multiple regression analyses determined that age, gender, ethnicity, and BMI were significantly associated with cognitive function in very late life.
Conclusions:
The results suggest that extreme values of body mass (low and high) in combination with normal BP (< 130 mmHg) are potential risk factors for compromised cognition.
DOI: https://doi.org/10.37349/emed.2023.00165
This article belongs to the special issue Determinants of Exceptional Longevity
Complex enzyme interactions play a role in the spread of cancer, a process fueled by unregulated cell proliferation. DNA topoisomerases, which are important for fixing DNA topological problems, have drawn a lot of interest as potential targets for anti-cancer medications. Cancer treatment, which includes radiation, surgery, and chemotherapy, tries to control cell survival, demise, and mobility, which are mediated by ion transportation across cell membranes via channels and carriers. The malignant transition is characterised by altered channels and carriers. Chemoresistance, which commonly develops after chemotherapy, denotes decreased therapeutic effectiveness against cancer progression. Chemosensitizers are used in combination with anti-cancer medications to overcome this resistance, particularly against adenosine triphosphate (ATP)-binding cassette (ABC) transporters including P-glycoprotein, multidrug resistance-associated protein 1 (MRP1), breast cancer resistance protein (BCRP). Effective targets for treatment are transcription factors, which play a key role in the development of cancer. With the use of interactions with receptors, enzymes, ion channels, transporters, and TFs, nanotechnology improves the safety of tumour localization, treatment, and diagnostics. As a result of mutations or altered signalling, rat sarcoma (RAS) proteins regulate signalling, which is essential for both healthy growth and the development of cancer. Rational treatments that target RAS pathways have the potential to inhibit the growth and spread of tumours. New treatments are still being developed, and they are showing promise in clinical settings. The roles of receptors on tumour cells, their significance for cancer therapy, and recent advancements in preclinical and clinical research are all included in this overview.
Complex enzyme interactions play a role in the spread of cancer, a process fueled by unregulated cell proliferation. DNA topoisomerases, which are important for fixing DNA topological problems, have drawn a lot of interest as potential targets for anti-cancer medications. Cancer treatment, which includes radiation, surgery, and chemotherapy, tries to control cell survival, demise, and mobility, which are mediated by ion transportation across cell membranes via channels and carriers. The malignant transition is characterised by altered channels and carriers. Chemoresistance, which commonly develops after chemotherapy, denotes decreased therapeutic effectiveness against cancer progression. Chemosensitizers are used in combination with anti-cancer medications to overcome this resistance, particularly against adenosine triphosphate (ATP)-binding cassette (ABC) transporters including P-glycoprotein, multidrug resistance-associated protein 1 (MRP1), breast cancer resistance protein (BCRP). Effective targets for treatment are transcription factors, which play a key role in the development of cancer. With the use of interactions with receptors, enzymes, ion channels, transporters, and TFs, nanotechnology improves the safety of tumour localization, treatment, and diagnostics. As a result of mutations or altered signalling, rat sarcoma (RAS) proteins regulate signalling, which is essential for both healthy growth and the development of cancer. Rational treatments that target RAS pathways have the potential to inhibit the growth and spread of tumours. New treatments are still being developed, and they are showing promise in clinical settings. The roles of receptors on tumour cells, their significance for cancer therapy, and recent advancements in preclinical and clinical research are all included in this overview.
DOI: https://doi.org/10.37349/emed.2023.00166
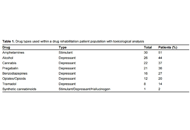
Diabetes mellitus has become increasingly more common and diagnosed within the global population. Coupled with the continued prevalence of substance use, there are some distinct considerations for users suffering (knowingly or unknowingly) from type 1 or type 2 diabetes. The various different types of drugs of abuse including central nervous system stimulants, depressants, and hallucinogens present varying direct and indirect complications for diabetes based on their physiological and psychological effects ranging from non-compliance with medication to an increased risk of hypoglycaemia, hyperglycaemia, and/or ketoacidosis. This perspective highlights these issues supported by the drug history and toxicological findings in patients undergoing drug rehabilitation in the United Arab Emirates (UAE) demonstrating the use of alcohol, amphetamines, benzodiazepines, cannabis, opiates/opioids (especially tramadol), pregabalin, and synthetic cannabinoids. Physicians and drug clinic professionals should be aware of the contraindications of substance use and diabetes with a view to educating patients and healthcare professionals within such clinical settings.
Diabetes mellitus has become increasingly more common and diagnosed within the global population. Coupled with the continued prevalence of substance use, there are some distinct considerations for users suffering (knowingly or unknowingly) from type 1 or type 2 diabetes. The various different types of drugs of abuse including central nervous system stimulants, depressants, and hallucinogens present varying direct and indirect complications for diabetes based on their physiological and psychological effects ranging from non-compliance with medication to an increased risk of hypoglycaemia, hyperglycaemia, and/or ketoacidosis. This perspective highlights these issues supported by the drug history and toxicological findings in patients undergoing drug rehabilitation in the United Arab Emirates (UAE) demonstrating the use of alcohol, amphetamines, benzodiazepines, cannabis, opiates/opioids (especially tramadol), pregabalin, and synthetic cannabinoids. Physicians and drug clinic professionals should be aware of the contraindications of substance use and diabetes with a view to educating patients and healthcare professionals within such clinical settings.
DOI: https://doi.org/10.37349/emed.2023.00167
This article belongs to the special issue The Biological Basis of Substance Use Disorders
Self-replicating RNA viruses such as alphaviruses, flaviviruses, paramyxoviruses, and rhabdoviruses have been engineered as expression vectors for vaccine development. The prominent feature of self-replicating RNA viruses is their RNA-dependent RNA polymerase activity, which generates massive self-amplification of RNA in the cytoplasm of infected host cells leading to extreme levels of transgene expression. Infectious diseases have been targeted by overexpression of surface proteins of pathogens as antigens for vaccine development. Moreover, overexpression of tumor-associated antigens and immunostimulatory genes has been the basis for cancer vaccines. Proof-of-concept of robust antigen-specific immune responses and protection against challenges with lethal doses of infectious agents have been demonstrated. Likewise, vaccine development against various cancers has elicited strong immune responses and resulted in tumor regression and eradication, cure, and prolonged survival in animal tumor models. Good safety and immune responses have been achieved in clinical trials. The ERVEBO® vaccine, based on the vesicular stomatitis virus, has been approved for immunization against the Ebola virus disease.
Self-replicating RNA viruses such as alphaviruses, flaviviruses, paramyxoviruses, and rhabdoviruses have been engineered as expression vectors for vaccine development. The prominent feature of self-replicating RNA viruses is their RNA-dependent RNA polymerase activity, which generates massive self-amplification of RNA in the cytoplasm of infected host cells leading to extreme levels of transgene expression. Infectious diseases have been targeted by overexpression of surface proteins of pathogens as antigens for vaccine development. Moreover, overexpression of tumor-associated antigens and immunostimulatory genes has been the basis for cancer vaccines. Proof-of-concept of robust antigen-specific immune responses and protection against challenges with lethal doses of infectious agents have been demonstrated. Likewise, vaccine development against various cancers has elicited strong immune responses and resulted in tumor regression and eradication, cure, and prolonged survival in animal tumor models. Good safety and immune responses have been achieved in clinical trials. The ERVEBO® vaccine, based on the vesicular stomatitis virus, has been approved for immunization against the Ebola virus disease.
DOI: https://doi.org/10.37349/emed.2023.00168
This article belongs to the special issue RNA World in Health and Disease
Bell’s palsy is a rapid unilateral peripheral paralysis of cranial nerve VII whose etiology is varied, most commonly associated with an acute infectious or inflammatory demyelinating process. Nerve injury can result in edema because of increased permeability of vascular structures, which can sometimes be seen as a locus of enhancement of magnetic resonance imaging (MRI). Bell’s palsy is typically considered a clinical diagnosis and the specificity and sensitivity of imaging have been poorly studied. Herein is describe a case of a 73-year-old male who presented to the emergency department with left-sided facial droop and no other focal neurological abnormalities. With a history of a Janus kinase 2 (JAK2) mutation and the new initial facial drooping, acute cerebrovascular insult was high on the differential. Initial labs and computerized tomography (CT) head were inconclusive, but MRI showed pronounced enhancement of the left distal internal carotid artery (ICA) with contiguous enhancement of the labyrinthine, geniculate, and tympanic segments of the left facial nerve. Diagnosing Bell’s palsy can be a challenge as there are numerous postulated etiologies stemming from trauma, infection, and neoplasm; with infection (particularly viral) postulated to be the most likely source. Though MRI is currently not validated as a tool in expediting Bell’s palsy diagnosis, findings such as the enhancement seen here provide some insight into the benefit of MRI as a diagnostic modality in some cases. This case is unique both for the diagnostic dilemma between stroke and Bell’s palsy and the potential for MRI imaging to help guide clinical decision-making into treatment.
Bell’s palsy is a rapid unilateral peripheral paralysis of cranial nerve VII whose etiology is varied, most commonly associated with an acute infectious or inflammatory demyelinating process. Nerve injury can result in edema because of increased permeability of vascular structures, which can sometimes be seen as a locus of enhancement of magnetic resonance imaging (MRI). Bell’s palsy is typically considered a clinical diagnosis and the specificity and sensitivity of imaging have been poorly studied. Herein is describe a case of a 73-year-old male who presented to the emergency department with left-sided facial droop and no other focal neurological abnormalities. With a history of a Janus kinase 2 (JAK2) mutation and the new initial facial drooping, acute cerebrovascular insult was high on the differential. Initial labs and computerized tomography (CT) head were inconclusive, but MRI showed pronounced enhancement of the left distal internal carotid artery (ICA) with contiguous enhancement of the labyrinthine, geniculate, and tympanic segments of the left facial nerve. Diagnosing Bell’s palsy can be a challenge as there are numerous postulated etiologies stemming from trauma, infection, and neoplasm; with infection (particularly viral) postulated to be the most likely source. Though MRI is currently not validated as a tool in expediting Bell’s palsy diagnosis, findings such as the enhancement seen here provide some insight into the benefit of MRI as a diagnostic modality in some cases. This case is unique both for the diagnostic dilemma between stroke and Bell’s palsy and the potential for MRI imaging to help guide clinical decision-making into treatment.
DOI: https://doi.org/10.37349/emed.2023.00169
Aim:
Parkinson’s disease (PD) is a complex, chronic neurodegenerative disorder with predominately sporadic etiology. Intricate genetic-environmental interactions lead to the hallmarks of the disease: degeneration of dopaminergic neurons and the deposition of α-synuclein aggregates. The aim of this study was to establish a novel primary patient cell model as an in vitro screen to study α-synuclein processing for drug screening.
Methods:
Primary patient olfactory neuroepithelial-derived cells (ONS) were exposed to α-synuclein and examined for cytotoxicity, processing, and solubility over 48 h. Epigallocatechin gallate (EGCG), which is known to destabilise α-synuclein fibrils, was used to investigate the solubilisation of α-synuclein in the model system.
Results:
Exposure to 0.1 μmol/L α-synuclein preformed fibrils was not toxic to ONS over 48 h. ONS processing of α-synuclein was observed to be different in PD cells by their increased accumulation in the cytoplasm. Processing deficits in the PD ONS were confirmed by immunoblotting with an increase in sodium dodecyl sulfate (SDS)-insoluble α-synuclein after 48 h.
Conclusions:
The data has illustrated the utility of primary patient ONS as a model system to understand the processing of α-synuclein. Considerable differences in α-synuclein processing were identified in PD ONS. Furthermore, the data suggests that primary patient ONS are a viable in vitro drug screening platform for α-synuclein pathology in PD.
Aim:
Parkinson’s disease (PD) is a complex, chronic neurodegenerative disorder with predominately sporadic etiology. Intricate genetic-environmental interactions lead to the hallmarks of the disease: degeneration of dopaminergic neurons and the deposition of α-synuclein aggregates. The aim of this study was to establish a novel primary patient cell model as an in vitro screen to study α-synuclein processing for drug screening.
Methods:
Primary patient olfactory neuroepithelial-derived cells (ONS) were exposed to α-synuclein and examined for cytotoxicity, processing, and solubility over 48 h. Epigallocatechin gallate (EGCG), which is known to destabilise α-synuclein fibrils, was used to investigate the solubilisation of α-synuclein in the model system.
Results:
Exposure to 0.1 μmol/L α-synuclein preformed fibrils was not toxic to ONS over 48 h. ONS processing of α-synuclein was observed to be different in PD cells by their increased accumulation in the cytoplasm. Processing deficits in the PD ONS were confirmed by immunoblotting with an increase in sodium dodecyl sulfate (SDS)-insoluble α-synuclein after 48 h.
Conclusions:
The data has illustrated the utility of primary patient ONS as a model system to understand the processing of α-synuclein. Considerable differences in α-synuclein processing were identified in PD ONS. Furthermore, the data suggests that primary patient ONS are a viable in vitro drug screening platform for α-synuclein pathology in PD.
DOI: https://doi.org/10.37349/emed.2023.00170
Aim:
Cannabis use for sleep-related problems is on the rise; however, little is known about the cannabis products people are using for sleep or the perceived effects of cannabis in comparison to more conventional sleep aids. Therefore, the aim of this study was to examine the products cannabis users prefer to use for sleep as well as their experiences with cannabis relative to more conventional sleep aids.
Methods:
De-identified archival data from a Strainprint® survey of 1,216 individuals who use cannabis for sleep were analyzed.
Results:
Participants predominantly reported smoking joints or vaping flower as their methods of administration, and seeking tetrahydrocannabinol (THC), cannabidiol (CBD), and the terpene myrcene in the cannabis they use for sleep. Only a small minority reported using cannabis in conjunction with conventional sleep aids. Comparisons of the self-reported effects of cannabis to conventional sleep aids revealed that participants reported feeling more refreshed, focused, better able to function, fewer headaches, and less nausea the morning after using cannabis for sleep than after using more conventional sleep aids or no sleep aids. However, they indicated they were more sleepy, anxious, and irritable in the mornings following the use of cannabis relative to other sleep aids. Participants were more likely to report red eyes and thirst and less likely to report nausea, anxiety, paranoia, and racing heart as side effects of cannabis relative to other sleep aids.
Conclusions:
Knowledge gained from this survey will provide health professionals with a better understanding of why people are using cannabis for sleep and may help guide future more controlled research.
Aim:
Cannabis use for sleep-related problems is on the rise; however, little is known about the cannabis products people are using for sleep or the perceived effects of cannabis in comparison to more conventional sleep aids. Therefore, the aim of this study was to examine the products cannabis users prefer to use for sleep as well as their experiences with cannabis relative to more conventional sleep aids.
Methods:
De-identified archival data from a Strainprint® survey of 1,216 individuals who use cannabis for sleep were analyzed.
Results:
Participants predominantly reported smoking joints or vaping flower as their methods of administration, and seeking tetrahydrocannabinol (THC), cannabidiol (CBD), and the terpene myrcene in the cannabis they use for sleep. Only a small minority reported using cannabis in conjunction with conventional sleep aids. Comparisons of the self-reported effects of cannabis to conventional sleep aids revealed that participants reported feeling more refreshed, focused, better able to function, fewer headaches, and less nausea the morning after using cannabis for sleep than after using more conventional sleep aids or no sleep aids. However, they indicated they were more sleepy, anxious, and irritable in the mornings following the use of cannabis relative to other sleep aids. Participants were more likely to report red eyes and thirst and less likely to report nausea, anxiety, paranoia, and racing heart as side effects of cannabis relative to other sleep aids.
Conclusions:
Knowledge gained from this survey will provide health professionals with a better understanding of why people are using cannabis for sleep and may help guide future more controlled research.
DOI: https://doi.org/10.37349/emed.2023.00171
This article belongs to the special issue Beyond Weed: Clinical Applications of Cannabis and Cannabinoids
