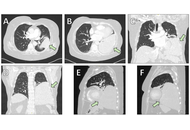












Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms that typically arise from the pleura but may occur in various extrathoracic sites. Primary intraparenchymal pulmonary SFTs without pleural attachment are exceptionally uncommon and often pose diagnostic and therapeutic challenges. We report the case of a middle-aged female patient presenting with progressive dyspnea and a large mass in the left lower lobe on imaging. Computed tomography revealed a well-circumscribed, hypervascular mass occupying the left lower lobe. Bronchoscopic and percutaneous biopsies were nondiagnostic, and surgical resection was pursued. Intraoperatively, the tumor was found to arise from the lung parenchyma without pleural involvement. Histopathological examination demonstrated a spindle-cell neoplasm with the typical “patternless pattern,” and immunohistochemistry confirmed nuclear STAT6 positivity, establishing the diagnosis of SFT. The postoperative course was uneventful apart from a transient pulmonary embolism, which was successfully treated. The patient was discharged in good condition and is under regular radiologic surveillance. SFTs of the lung are rare and often mimic more common pulmonary tumors radiologically. Histologic confirmation with STAT6 immunohistochemistry is crucial for accurate diagnosis. Complete surgical excision remains the mainstay of treatment. Given the risk of late recurrence—especially in large tumors—long-term imaging follow-up is mandatory. This case highlights the importance of considering SFT in the differential diagnosis of large pulmonary masses, the critical role of STAT6-based histopathologic confirmation, and the necessity for prolonged surveillance even after complete resection.
Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms that typically arise from the pleura but may occur in various extrathoracic sites. Primary intraparenchymal pulmonary SFTs without pleural attachment are exceptionally uncommon and often pose diagnostic and therapeutic challenges. We report the case of a middle-aged female patient presenting with progressive dyspnea and a large mass in the left lower lobe on imaging. Computed tomography revealed a well-circumscribed, hypervascular mass occupying the left lower lobe. Bronchoscopic and percutaneous biopsies were nondiagnostic, and surgical resection was pursued. Intraoperatively, the tumor was found to arise from the lung parenchyma without pleural involvement. Histopathological examination demonstrated a spindle-cell neoplasm with the typical “patternless pattern,” and immunohistochemistry confirmed nuclear STAT6 positivity, establishing the diagnosis of SFT. The postoperative course was uneventful apart from a transient pulmonary embolism, which was successfully treated. The patient was discharged in good condition and is under regular radiologic surveillance. SFTs of the lung are rare and often mimic more common pulmonary tumors radiologically. Histologic confirmation with STAT6 immunohistochemistry is crucial for accurate diagnosis. Complete surgical excision remains the mainstay of treatment. Given the risk of late recurrence—especially in large tumors—long-term imaging follow-up is mandatory. This case highlights the importance of considering SFT in the differential diagnosis of large pulmonary masses, the critical role of STAT6-based histopathologic confirmation, and the necessity for prolonged surveillance even after complete resection.
DOI: https://doi.org/10.37349/etat.2026.1002367
Aim:
DNA damage involves in the carcinogenesis of some cancer and may act as a target for therapeutic intervention of cancers. However, it is unclear whether aflatoxin B1 (AFB1)-DNA adducts (ADAs), an important kind of DNA damage caused by AFB1, affect the efficiency of post-operative adjuvant transarterial chemoembolization (po-TACE) treatment improving hepatocellular carcinoma (HCC) survival.
Methods:
A hospital-based retrospective study, including 318 patients with Barcelona Clinic Liver Cancer (BCLC)-C stage HCC from high AFB1 exposure areas, to investigate the potential effects of ADAs in the tissues with HCC on po-TACE treatment. The amount of ADAs in the cancerous tissues was tested by competitive enzyme-linked immunosorbent assay (c-ELISA).
Results:
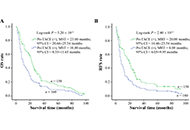
Among these patients with HCC, the average amount of ADAs was 3.00 µmol/mol ± 1.51 µmol/mol DNA in their tissues with cancer. For these patients, increasing amount of ADAs was significantly associated with poorer overall survival (OS) and tumor reoccurrence-free survival (RFS), with corresponding death risk (DR) of 3.69 (2.78–4.91) and tumor recurrence risk (TRR) of 2.95 (2.24–3.88). The po-TACE therapy can efficiently improve their prognosis [DR = 0.59 (0.46–0.76), TRR = 0.63 (0.49–0.82)]. Interestingly, this improving role was more noticeable among these patients with high ADAs [DR = 0.36 (0.24–0.53), TRR = 0.40 (0.28–0.59)], but not among those with low ADAs (P > 0.05).
Conclusions:
These results suggest that increasing ADAs in the cancerous tissues may be beneficial for po-TACE in ameliorating the survival of patients with HCC.
Aim:
DNA damage involves in the carcinogenesis of some cancer and may act as a target for therapeutic intervention of cancers. However, it is unclear whether aflatoxin B1 (AFB1)-DNA adducts (ADAs), an important kind of DNA damage caused by AFB1, affect the efficiency of post-operative adjuvant transarterial chemoembolization (po-TACE) treatment improving hepatocellular carcinoma (HCC) survival.
Methods:
A hospital-based retrospective study, including 318 patients with Barcelona Clinic Liver Cancer (BCLC)-C stage HCC from high AFB1 exposure areas, to investigate the potential effects of ADAs in the tissues with HCC on po-TACE treatment. The amount of ADAs in the cancerous tissues was tested by competitive enzyme-linked immunosorbent assay (c-ELISA).
Results:
Among these patients with HCC, the average amount of ADAs was 3.00 µmol/mol ± 1.51 µmol/mol DNA in their tissues with cancer. For these patients, increasing amount of ADAs was significantly associated with poorer overall survival (OS) and tumor reoccurrence-free survival (RFS), with corresponding death risk (DR) of 3.69 (2.78–4.91) and tumor recurrence risk (TRR) of 2.95 (2.24–3.88). The po-TACE therapy can efficiently improve their prognosis [DR = 0.59 (0.46–0.76), TRR = 0.63 (0.49–0.82)]. Interestingly, this improving role was more noticeable among these patients with high ADAs [DR = 0.36 (0.24–0.53), TRR = 0.40 (0.28–0.59)], but not among those with low ADAs (P > 0.05).
Conclusions:
These results suggest that increasing ADAs in the cancerous tissues may be beneficial for po-TACE in ameliorating the survival of patients with HCC.
DOI: https://doi.org/10.37349/etat.2023.00167
Artificial intelligence (AI) algorithms have been applied in abundant medical tasks with high accuracy and efficiency. Physicians can improve their diagnostic efficiency with the assistance of AI techniques for improving the subsequent personalized treatment and surveillance. AI algorithms fundamentally capture data, identify underlying patterns, achieve preset endpoints, and provide decisions and predictions about real-world events with working principles of machine learning and deep learning. AI algorithms with sufficient graphic processing unit power have been demonstrated to provide timely diagnostic references based on preliminary training of large amounts of clinical and imaging data. The sample size issue is an inevitable challenge for pediatric oncology considering its low morbidity and individual heterogeneity. However, this problem may be solved in the near future considering the exponential advancements of AI algorithms technically to decrease the dependence of AI operation on the amount of data sets and the efficiency of computing power. For instance, it could be a feasible solution by shifting convolutional neural networks (CNNs) from adults and sharing CNN algorithms across multiple institutions besides original data. The present review provides important insights into emerging AI applications for the diagnosis of pediatric oncology by systematically overviewing of up-to-date literature.
Artificial intelligence (AI) algorithms have been applied in abundant medical tasks with high accuracy and efficiency. Physicians can improve their diagnostic efficiency with the assistance of AI techniques for improving the subsequent personalized treatment and surveillance. AI algorithms fundamentally capture data, identify underlying patterns, achieve preset endpoints, and provide decisions and predictions about real-world events with working principles of machine learning and deep learning. AI algorithms with sufficient graphic processing unit power have been demonstrated to provide timely diagnostic references based on preliminary training of large amounts of clinical and imaging data. The sample size issue is an inevitable challenge for pediatric oncology considering its low morbidity and individual heterogeneity. However, this problem may be solved in the near future considering the exponential advancements of AI algorithms technically to decrease the dependence of AI operation on the amount of data sets and the efficiency of computing power. For instance, it could be a feasible solution by shifting convolutional neural networks (CNNs) from adults and sharing CNN algorithms across multiple institutions besides original data. The present review provides important insights into emerging AI applications for the diagnosis of pediatric oncology by systematically overviewing of up-to-date literature.
DOI: https://doi.org/10.37349/etat.2023.00127
This article belongs to the special issue Artificial Intelligence for Precision Oncology
Aim:
This study was designed to investigate the anticancer efficacy of the organic leaf extracts of the plant, Plectranthus vettiveroides (P. vettiveroides), and to analyze the molecular mechanism of the anticancer activity.
Methods:
The leaf extracts were prepared by polarity-graded serial extraction of the dried leaf powder. The cytotoxic effect of the extracts was analyzed by the 3-(4, 5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT) assay. The most active ethyl acetate extract was subjected to bioactivity-guided fractionation by column chromatography, which yielded a cytotoxic fraction designated as the P. vettiveroides fraction (PVF). The anticancer property of PVF was confirmed further by clonogenic assay. The mechanism of PVF-induced cell death was analyzed by flow cytometry and fluorescence microscopy. Additionally, the effects of PVF on apoptotic and cell survival pathways were analyzed using western immunoblot analysis.
Results:
A bioactive fraction PVF, was isolated from the ethyl acetate leaf extract. PVF showed significant anticancer activity against colon cancer cells, whilst normal cells were comparatively less affected. PVF induced strong apoptotic stimuli in colorectal carcinoma cell line HCT116, involving both extrinsic and intrinsic pathways. Investigation into the molecular mechanism of anticancer activity of PVF in HCT116 cells revealed that the fraction activates the pro-apoptotic pathway via tumor suppressor protein 53 (p53) and inhibits the anti-apoptotic pathway by regulating phosphatidylinositol 3-kinase (PI3K) signaling.
Conclusions:
The findings of this study demonstrate, with mechanism-based evidence, the chemotherapeutic potential of a bioactive fraction PVF, derived from the leaves of the medicinal plant P. vettiveroides against colon cancer.
Aim:
This study was designed to investigate the anticancer efficacy of the organic leaf extracts of the plant, Plectranthus vettiveroides (P. vettiveroides), and to analyze the molecular mechanism of the anticancer activity.
Methods:
The leaf extracts were prepared by polarity-graded serial extraction of the dried leaf powder. The cytotoxic effect of the extracts was analyzed by the 3-(4, 5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT) assay. The most active ethyl acetate extract was subjected to bioactivity-guided fractionation by column chromatography, which yielded a cytotoxic fraction designated as the P. vettiveroides fraction (PVF). The anticancer property of PVF was confirmed further by clonogenic assay. The mechanism of PVF-induced cell death was analyzed by flow cytometry and fluorescence microscopy. Additionally, the effects of PVF on apoptotic and cell survival pathways were analyzed using western immunoblot analysis.
Results:
A bioactive fraction PVF, was isolated from the ethyl acetate leaf extract. PVF showed significant anticancer activity against colon cancer cells, whilst normal cells were comparatively less affected. PVF induced strong apoptotic stimuli in colorectal carcinoma cell line HCT116, involving both extrinsic and intrinsic pathways. Investigation into the molecular mechanism of anticancer activity of PVF in HCT116 cells revealed that the fraction activates the pro-apoptotic pathway via tumor suppressor protein 53 (p53) and inhibits the anti-apoptotic pathway by regulating phosphatidylinositol 3-kinase (PI3K) signaling.
Conclusions:
The findings of this study demonstrate, with mechanism-based evidence, the chemotherapeutic potential of a bioactive fraction PVF, derived from the leaves of the medicinal plant P. vettiveroides against colon cancer.
DOI: https://doi.org/10.37349/etat.2023.00131
This article belongs to the special issue Plant Extracts as an Infinite Resource for New Anticancer Agents
Aim:
AT-rich interaction domain 1A (ARID1A) encodes a key component of the SWItch/Sucrose Non-Fermentable (SWI/SNF) chromatin remodeling complex that participates in gene expression. ARID1A alterations are quite common among cancer patients, although their role remains debated. The aim of this article was to study ARID1A-mutated cancer patients.
Methods:
Molecular and clinical data of cancer patients evaluated at Phase 1 Unit of Fondazione Policlinico Universitario A. Gemelli IRCCS were collected. Molecular analyses were performed using FoundationOne® CDx (Foundation Medicine Inc., Cambridge, MA, United States). Cancer patients with at least one molecular alteration in ARID1A gene were identified as ARID1A+.
Results:
Among the 270 patients undergoing molecular analysis, we found 25 (9%) with at least one pathogenic alteration in ARID1A. The vast majority of these patients were female (84%). The median age at diagnosis was 59; most of the cancers (15, 60%) were gynecological (especially endometrioid endometrial cancers and clear cell ovarian cancers), diagnosed at an early stage. Frameshift alterations in ARID1A were the most common (19/31, 61%) alterations. The median number of mutations in ARID1A+ population was higher compared to ARID1A– population (6 vs. 4), as well as tumor mutational burden (TMB) [20 mutations/megabase (mut/Mb) vs. 1.26 mut/Mb]. Phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA), phosphatase and tensin homolog (PTEN), catenin beta 1 (CTNNB1), and lysine methyltransferase 2D (MLL2) mutations were enriched in ARID1A+ population. In this cohort, ARID1A did not display any relation with response to platinum chemotherapy. Cancers with double alterations in ARID1A (ARID1A2+) were all gynecological cancers (83% endometrioid endometrial cancers).
Conclusions:
This analysis provides clinical and molecular details about the phenotypes of ARID1A+ cancers, in particular the subgroup of gynecologic cancers. The high frequency of concurrent mutations in the phosphoinositide 3-kinase (PI3K) pathway among endometrioid endometrial cancers may support the proposal of a new treatment strategy based on the combination of ataxia telangiectasia and Rad3-related (ATR) inhibitor and PIK3CA inhibitor.
Aim:
AT-rich interaction domain 1A (ARID1A) encodes a key component of the SWItch/Sucrose Non-Fermentable (SWI/SNF) chromatin remodeling complex that participates in gene expression. ARID1A alterations are quite common among cancer patients, although their role remains debated. The aim of this article was to study ARID1A-mutated cancer patients.
Methods:
Molecular and clinical data of cancer patients evaluated at Phase 1 Unit of Fondazione Policlinico Universitario A. Gemelli IRCCS were collected. Molecular analyses were performed using FoundationOne® CDx (Foundation Medicine Inc., Cambridge, MA, United States). Cancer patients with at least one molecular alteration in ARID1A gene were identified as ARID1A+.
Results:
Among the 270 patients undergoing molecular analysis, we found 25 (9%) with at least one pathogenic alteration in ARID1A. The vast majority of these patients were female (84%). The median age at diagnosis was 59; most of the cancers (15, 60%) were gynecological (especially endometrioid endometrial cancers and clear cell ovarian cancers), diagnosed at an early stage. Frameshift alterations in ARID1A were the most common (19/31, 61%) alterations. The median number of mutations in ARID1A+ population was higher compared to ARID1A– population (6 vs. 4), as well as tumor mutational burden (TMB) [20 mutations/megabase (mut/Mb) vs. 1.26 mut/Mb]. Phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA), phosphatase and tensin homolog (PTEN), catenin beta 1 (CTNNB1), and lysine methyltransferase 2D (MLL2) mutations were enriched in ARID1A+ population. In this cohort, ARID1A did not display any relation with response to platinum chemotherapy. Cancers with double alterations in ARID1A (ARID1A2+) were all gynecological cancers (83% endometrioid endometrial cancers).
Conclusions:
This analysis provides clinical and molecular details about the phenotypes of ARID1A+ cancers, in particular the subgroup of gynecologic cancers. The high frequency of concurrent mutations in the phosphoinositide 3-kinase (PI3K) pathway among endometrioid endometrial cancers may support the proposal of a new treatment strategy based on the combination of ataxia telangiectasia and Rad3-related (ATR) inhibitor and PIK3CA inhibitor.
DOI: https://doi.org/10.37349/etat.2023.00163
Interferon (IFN)-stimulated gene 15 (ISG15) is a member of the ubiquitin-like (UBL) protein family that can modify specific proteins via a catalytic process called ISGylation. This posttranslational modification can modulate the stability of the ISGylated proteins and protein-protein interactions. Some proteins modified by ISG15 have been identified in malignant neoplasms, suggesting the functional relevance of ISGylation in cancer. This review discusses the ISGylated proteins reported in malignant neoplasms that suggest the potential of ISG15 as a biomarker and therapeutic target in cancer.
Interferon (IFN)-stimulated gene 15 (ISG15) is a member of the ubiquitin-like (UBL) protein family that can modify specific proteins via a catalytic process called ISGylation. This posttranslational modification can modulate the stability of the ISGylated proteins and protein-protein interactions. Some proteins modified by ISG15 have been identified in malignant neoplasms, suggesting the functional relevance of ISGylation in cancer. This review discusses the ISGylated proteins reported in malignant neoplasms that suggest the potential of ISG15 as a biomarker and therapeutic target in cancer.
DOI: https://doi.org/10.37349/etat.2023.00162
This article belongs to the special issue Posttranslational Modifications in Health and Disease
Aim:
Delineate structure-based inhibition of colony-stimulating factor-1 receptor (CSF1R) by small molecule CSF1R inhibitors in clinical development for target identification and potential lead optimization in cancer therapeutics since CSF1R is a novel predictive biomarker for immunotherapy in cancer.
Methods:
Compounds were in silico modelled by induced fit docking protocol in a molecular operating environment (MOE, MOE.v.2015). The 3-dimensional (3D) X-ray crystallized structure of CSF1R kinase (Protein Databank, ID 4R7H) was obtained from Research Collaboratory for Structural Bioinformatics (RSCB) Protein Databank. The 3D conformers of edicotinib, DCC-3014, ARRY-382, BLZ-945, chiauranib, dovitinib, and sorafenib were obtained from PubChem Database. These structures were modelled in Amber10:EHT molecular force field, and quick prep application was used to correct and optimize the structures for missing residues, H-counts, termini capping, and alternates. The binding site was defined within the vicinity of the co-crystallized ligand of CSF1R kinase. The compounds were docked by the triangular matcher placement method and ranked by the London dG scoring function. The docked poses were further refined by the induced fit method. The pose with the lowest binding score (ΔG) was used to model the ligand interaction profile in Discovery Studio Visualizer v17.2. The co-crystallized ligand was docked in its apo conformation, and root-mean-square deviation was computed to validate the docking protocol.
Results:
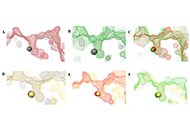
All 7 CSF1R inhibitors interact with residue Met637 exhibiting selectivity except for edicotinib. The inhibitors maintain CSF1R in an auto-inhibitory conformation by interacting with Asp797 of the Asp-Phe-Gly (DFG) motif and/or hindering the conserved salt bridge formed between Glu633 and Lys616 thus stabilizing the activation loop, or interacting with tryptophan residue (Trp550) in the juxtamembrane domain. DCC-3014, ARRY-382, BLZ-945, and sorafenib bind with the lowest binding energy with CSF1R kinase.
Conclusions:
Pyrimidines are potent inhibitors that interact with CSF1R residues. DCC-3014 and ARRY-382 exhibit exceptional pharmaceutical potential exhibiting great structural stability and affinity.
Aim:
Delineate structure-based inhibition of colony-stimulating factor-1 receptor (CSF1R) by small molecule CSF1R inhibitors in clinical development for target identification and potential lead optimization in cancer therapeutics since CSF1R is a novel predictive biomarker for immunotherapy in cancer.
Methods:
Compounds were in silico modelled by induced fit docking protocol in a molecular operating environment (MOE, MOE.v.2015). The 3-dimensional (3D) X-ray crystallized structure of CSF1R kinase (Protein Databank, ID 4R7H) was obtained from Research Collaboratory for Structural Bioinformatics (RSCB) Protein Databank. The 3D conformers of edicotinib, DCC-3014, ARRY-382, BLZ-945, chiauranib, dovitinib, and sorafenib were obtained from PubChem Database. These structures were modelled in Amber10:EHT molecular force field, and quick prep application was used to correct and optimize the structures for missing residues, H-counts, termini capping, and alternates. The binding site was defined within the vicinity of the co-crystallized ligand of CSF1R kinase. The compounds were docked by the triangular matcher placement method and ranked by the London dG scoring function. The docked poses were further refined by the induced fit method. The pose with the lowest binding score (ΔG) was used to model the ligand interaction profile in Discovery Studio Visualizer v17.2. The co-crystallized ligand was docked in its apo conformation, and root-mean-square deviation was computed to validate the docking protocol.
Results:
All 7 CSF1R inhibitors interact with residue Met637 exhibiting selectivity except for edicotinib. The inhibitors maintain CSF1R in an auto-inhibitory conformation by interacting with Asp797 of the Asp-Phe-Gly (DFG) motif and/or hindering the conserved salt bridge formed between Glu633 and Lys616 thus stabilizing the activation loop, or interacting with tryptophan residue (Trp550) in the juxtamembrane domain. DCC-3014, ARRY-382, BLZ-945, and sorafenib bind with the lowest binding energy with CSF1R kinase.
Conclusions:
Pyrimidines are potent inhibitors that interact with CSF1R residues. DCC-3014 and ARRY-382 exhibit exceptional pharmaceutical potential exhibiting great structural stability and affinity.
DOI: https://doi.org/10.37349/etat.2023.00164
Aim:
In renal cell carcinoma (RCC), tumor heterogeneity generated challenges to biomarker development and therapeutic management, often becoming responsible for primary and acquired drug resistance. This study aimed to assess the inter-tumoral, intra-tumoral, and intra-lesional heterogeneity of known druggable targets in metastatic RCC (mRCC).
Methods:
The RIVELATOR study was a monocenter retrospective analysis of biological samples from 25 cases of primary RCC and their paired pulmonary metastases. The biomarkers analyzed included MET, mTOR, PD-1/PD-L1 pathways and the immune context.
Results:
High multi-level heterogeneity was demonstrated. MET was the most reliable biomarker, with the lowest intratumor heterogeneity: the positive mutual correlation between MET expression in primary tumors and their metastases had a significantly proportional intensity (P = 0.038). The intratumor heterogeneity grade was significantly higher for the mTOR pathway proteins. Combined immunophenotypical expression patterns and their correlations with the immune context were uncovered [i.e., mTOR expression in the metastases positively correlated with PD-L1 expression in tumor-infiltrating lymphocytes (TILs), P = 0.019; MET expression was related to PD-1 expression on TILs (P = 0.041, ρ = 0.41) and peritumoral lymphocytes (RILs; P = 0.013, ρ = 0.49)], suggesting the possibility of predicting drug response or resistance to tyrosine kinase, mTOR, or immune checkpoint inhibitors.
Conclusions:
In mRCC, multiple and multi-level assays of potentially predictive biomarkers are needed for their reliable translation into clinical practice. The easy-to-use immunohistochemical method of the present study allowed the identification of different combined expression patterns, providing cues for planning the management of systemic treatment combinations and sequences in an mRCC patient population. The quantitative heterogeneity of the investigated biomarkers suggests that multiple intralesional assays are needed to consider the assessment reliable for clinical considerations.
Aim:
In renal cell carcinoma (RCC), tumor heterogeneity generated challenges to biomarker development and therapeutic management, often becoming responsible for primary and acquired drug resistance. This study aimed to assess the inter-tumoral, intra-tumoral, and intra-lesional heterogeneity of known druggable targets in metastatic RCC (mRCC).
Methods:
The RIVELATOR study was a monocenter retrospective analysis of biological samples from 25 cases of primary RCC and their paired pulmonary metastases. The biomarkers analyzed included MET, mTOR, PD-1/PD-L1 pathways and the immune context.
Results:
High multi-level heterogeneity was demonstrated. MET was the most reliable biomarker, with the lowest intratumor heterogeneity: the positive mutual correlation between MET expression in primary tumors and their metastases had a significantly proportional intensity (P = 0.038). The intratumor heterogeneity grade was significantly higher for the mTOR pathway proteins. Combined immunophenotypical expression patterns and their correlations with the immune context were uncovered [i.e., mTOR expression in the metastases positively correlated with PD-L1 expression in tumor-infiltrating lymphocytes (TILs), P = 0.019; MET expression was related to PD-1 expression on TILs (P = 0.041, ρ = 0.41) and peritumoral lymphocytes (RILs; P = 0.013, ρ = 0.49)], suggesting the possibility of predicting drug response or resistance to tyrosine kinase, mTOR, or immune checkpoint inhibitors.
Conclusions:
In mRCC, multiple and multi-level assays of potentially predictive biomarkers are needed for their reliable translation into clinical practice. The easy-to-use immunohistochemical method of the present study allowed the identification of different combined expression patterns, providing cues for planning the management of systemic treatment combinations and sequences in an mRCC patient population. The quantitative heterogeneity of the investigated biomarkers suggests that multiple intralesional assays are needed to consider the assessment reliable for clinical considerations.
DOI: https://doi.org/10.37349/etat.2023.00165
Histone deacetylases (HDACs) are a class of zinc (Zn)-dependent metalloenzymes that are responsible for epigenetic modifications. HDACs are largely associated with histone proteins that regulate gene expression at the DNA level. This tight regulation is controlled by acetylation [via histone acetyl transferases (HATs)] and deacetylation (via HDACs) of histone and non-histone proteins that alter the coiling state of DNA, thus impacting gene expression as a downstream effect. For the last two decades, HDACs have been studied extensively and indicated in a range of diseases where HDAC dysregulation has been strongly correlated with disease emergence and progression—most prominently, cancer, neurodegenerative diseases, HIV, and inflammatory diseases. The involvement of HDACs as regulators in these biochemical pathways established them as an attractive therapeutic target. This review summarizes the drug development efforts exerted to create HDAC inhibitors (HDACis), specifically class I HDACs, with a focus on the medicinal chemistry, structural design, and pharmacology aspects of these inhibitors.
Histone deacetylases (HDACs) are a class of zinc (Zn)-dependent metalloenzymes that are responsible for epigenetic modifications. HDACs are largely associated with histone proteins that regulate gene expression at the DNA level. This tight regulation is controlled by acetylation [via histone acetyl transferases (HATs)] and deacetylation (via HDACs) of histone and non-histone proteins that alter the coiling state of DNA, thus impacting gene expression as a downstream effect. For the last two decades, HDACs have been studied extensively and indicated in a range of diseases where HDAC dysregulation has been strongly correlated with disease emergence and progression—most prominently, cancer, neurodegenerative diseases, HIV, and inflammatory diseases. The involvement of HDACs as regulators in these biochemical pathways established them as an attractive therapeutic target. This review summarizes the drug development efforts exerted to create HDAC inhibitors (HDACis), specifically class I HDACs, with a focus on the medicinal chemistry, structural design, and pharmacology aspects of these inhibitors.
DOI: https://doi.org/10.37349/etat.2023.00166
This article belongs to the special issue Posttranslational Modifications in Health and Disease
Aim:
From the start of the pandemic, several aspects of healthcare policies changed, not least the clinical trials management from recruiting capabilities to the protocol compliance in terms of schedule of procedures, follow-up visits, staff constraints and monitoring. This study aims to assess the impact of the COronaVIrusDisease-2019 (COVID-19) pandemic in the conduction of clinical trials at the site of clinical oncology, Ancona (Italy), to identify the strengths and weaknesses upfront the past emergency, and to select better strategies for future similar situations.
Methods:
Data from February to July of the years 2019, 2020 and 2021 were collected and three practical parameters of the trial unit were investigated: milestones, performance, and impact.
Results:
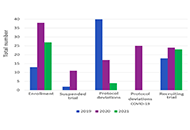
The trials mean numbers were 18, 24, and 23, in 2019, 2020, and 2021 respectively. The pre-Site Initiation Visit (PRE-SIV) rate grew from 66.6% in 2019 to 95.5% in 2021 with a deflection in 2020. Protocol deviations were 40 in the period February-July 2019, in the same period of 2020 the number of deviations increased due to COVID related ones, then there was a significant total decrease in February-July 2021. In 2020 and 2021, all the investigator meetings were online.
Conclusions:
The growing number of remote Site Initiation Visit (SIV) and meetings over the last 3 years suggests the feasibility of the on-line processes. The significant reduction in protocol deviations during 2021 is probably due to an under check of data during a pandemic. But that is also a possible key indicator of the coping strategy made out by clinical oncology to guarantee the continuity of care in clinical trials and to offer new opportunities of cancer care in a bad scenario such as a pandemic one.
Aim:
From the start of the pandemic, several aspects of healthcare policies changed, not least the clinical trials management from recruiting capabilities to the protocol compliance in terms of schedule of procedures, follow-up visits, staff constraints and monitoring. This study aims to assess the impact of the COronaVIrusDisease-2019 (COVID-19) pandemic in the conduction of clinical trials at the site of clinical oncology, Ancona (Italy), to identify the strengths and weaknesses upfront the past emergency, and to select better strategies for future similar situations.
Methods:
Data from February to July of the years 2019, 2020 and 2021 were collected and three practical parameters of the trial unit were investigated: milestones, performance, and impact.
Results:
The trials mean numbers were 18, 24, and 23, in 2019, 2020, and 2021 respectively. The pre-Site Initiation Visit (PRE-SIV) rate grew from 66.6% in 2019 to 95.5% in 2021 with a deflection in 2020. Protocol deviations were 40 in the period February-July 2019, in the same period of 2020 the number of deviations increased due to COVID related ones, then there was a significant total decrease in February-July 2021. In 2020 and 2021, all the investigator meetings were online.
Conclusions:
The growing number of remote Site Initiation Visit (SIV) and meetings over the last 3 years suggests the feasibility of the on-line processes. The significant reduction in protocol deviations during 2021 is probably due to an under check of data during a pandemic. But that is also a possible key indicator of the coping strategy made out by clinical oncology to guarantee the continuity of care in clinical trials and to offer new opportunities of cancer care in a bad scenario such as a pandemic one.
DOI: https://doi.org/10.37349/etat.2023.00168
This article belongs to the special issue COVID-19 and Cancer
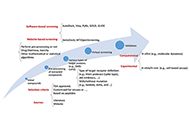
Malignant tumors of the external auditory canal (EAC) are rare neoplasms that appear in the head and neck area. A common feature of these malignancies is their rarity, as well as their delayed diagnosis due to the appearance of non-specific symptoms that mimic various benign otologic conditions. The reported histological types of cancer of the external ear are: squamous cell carcinoma, basal cell carcinoma, malignant melanoma, Merkel cell carcinoma, angiosarcoma, adnexal carcinoma (including ceruminous adenocarcinoma and adenoid cystic carcinoma), and lymphoma (Lancet Oncol. 2005;6:411–20. doi: 10.1016/S1470-2045(05)70208-4). Several therapeutic interventions have been proposed, primarily orientated towards the cure of the patient, placing the surgical excision of the lesions at the tip of the spear. Subsequently and depending on the clinical stage and the pathological characteristics of the tumor, radiation, chemotherapy, a combination thereof, or some form of palliative treatment for particularly advanced cases, may be recommended. The aim of all the above-mentioned approaches is the complete resection of the mass with negative surgical margins along with lymph node dissection, the elimination of any residual disease or metastasis, and the improvement of survival. The anatomical complexity of the region will always remain a demanding challenge. Nevertheless, advances in the fields of ear microsurgery, imaging, radiation, molecular biology, and genomics have led to remarkable outcomes compared to the past, with a view to the patient’s quality of life. Large, well-organized, and prospective studies with the participation of multiple centers in contrast to existing retrospective studies with a limited number of patients will help to establish universally accepted guidelines. The exploration of the molecular and genetic background of these cancers in conjunction with the search for new biomarkers and target molecules seems promising for providing upgraded and more personalized treatment modalities for the future.
Malignant tumors of the external auditory canal (EAC) are rare neoplasms that appear in the head and neck area. A common feature of these malignancies is their rarity, as well as their delayed diagnosis due to the appearance of non-specific symptoms that mimic various benign otologic conditions. The reported histological types of cancer of the external ear are: squamous cell carcinoma, basal cell carcinoma, malignant melanoma, Merkel cell carcinoma, angiosarcoma, adnexal carcinoma (including ceruminous adenocarcinoma and adenoid cystic carcinoma), and lymphoma (Lancet Oncol. 2005;6:411–20. doi: 10.1016/S1470-2045(05)70208-4). Several therapeutic interventions have been proposed, primarily orientated towards the cure of the patient, placing the surgical excision of the lesions at the tip of the spear. Subsequently and depending on the clinical stage and the pathological characteristics of the tumor, radiation, chemotherapy, a combination thereof, or some form of palliative treatment for particularly advanced cases, may be recommended. The aim of all the above-mentioned approaches is the complete resection of the mass with negative surgical margins along with lymph node dissection, the elimination of any residual disease or metastasis, and the improvement of survival. The anatomical complexity of the region will always remain a demanding challenge. Nevertheless, advances in the fields of ear microsurgery, imaging, radiation, molecular biology, and genomics have led to remarkable outcomes compared to the past, with a view to the patient’s quality of life. Large, well-organized, and prospective studies with the participation of multiple centers in contrast to existing retrospective studies with a limited number of patients will help to establish universally accepted guidelines. The exploration of the molecular and genetic background of these cancers in conjunction with the search for new biomarkers and target molecules seems promising for providing upgraded and more personalized treatment modalities for the future.
DOI: https://doi.org/10.37349/etat.2023.00169
This article belongs to the special issue Biomarkers for Personalized and Precise Cancer Diagnosis and Treatment
From attributing mutations to cancers with the advent of cutting-edge genetic technology in recent decades, to re-searching the age-old theory of intrinsic metabolic shift of cancers (Warburg’s glycolysis), the quest for a precise panacea for mainly the metastatic cancers, remains incessant. This review delineates the advanced glycation end product (AGE)-receptor for AGE (RAGE) pathway driven intricate oncogenic cues, budding from the metabolic (glycolytic) reliance of tumour cells, branching into metastatic emergence of malignancies. Strong AGE-RAGE concomitance in metastasis, chemo-resistance and cancer resurgence adversely incite disease progression and patient mortality. At the conjunction of metabolic and metastatic shift of cancers, are the “glycolytically” generated AGEs and AGE-activated RAGE, instigating aberrant molecular pathways, culminating in aggressive malignancies. AGEs as by-products of metabolic insurgence, modify the metabolome, epigenome and microbiome, besides coercing the inter-, intra- and extra-cellular micro-milieu conducive for oncogenic events like epithelial-mesenchymal transition (EMT). AGE-RAGE synergistically elicit ATP surge for surplus energy, autophagy for apoptotic evasion and chemo-resistance, insulin-like growth factor 1 (IGF-1) for meta-inflammation and angiogenesis, high mobility group box-1 (HMGB1) for immune tolerance, S100 proteins for metastasis, and p53 protein attenuation for tumour suppression. AGEs are pronouncedly reported in invasive forms of breast, prostate, colon and pancreatic cancers, higher in patients with cancer than healthy counterparts, and higher in advanced stage than localized phase. Hence, the investigation of person-specific presence of AGEs, soluble RAGE and AGE-activated RAGE can be advocated as impending bio-markers for diagnostic, prognostic and therapeutic purposes, to predict cancer risk in patients with diabetes, obesity, metabolic syndrome as well as general population, to monitor prognosis and metastasis in patients with cancer, and to reckon complications in cancer survivors. Furthermore, clinical reports of exogenous (dietary) and endogenous (internally formed) AGEs in cancer patients, and contemporary clinical trials involving AGE-RAGE axis in cancer are underlined with theranostic implications.
From attributing mutations to cancers with the advent of cutting-edge genetic technology in recent decades, to re-searching the age-old theory of intrinsic metabolic shift of cancers (Warburg’s glycolysis), the quest for a precise panacea for mainly the metastatic cancers, remains incessant. This review delineates the advanced glycation end product (AGE)-receptor for AGE (RAGE) pathway driven intricate oncogenic cues, budding from the metabolic (glycolytic) reliance of tumour cells, branching into metastatic emergence of malignancies. Strong AGE-RAGE concomitance in metastasis, chemo-resistance and cancer resurgence adversely incite disease progression and patient mortality. At the conjunction of metabolic and metastatic shift of cancers, are the “glycolytically” generated AGEs and AGE-activated RAGE, instigating aberrant molecular pathways, culminating in aggressive malignancies. AGEs as by-products of metabolic insurgence, modify the metabolome, epigenome and microbiome, besides coercing the inter-, intra- and extra-cellular micro-milieu conducive for oncogenic events like epithelial-mesenchymal transition (EMT). AGE-RAGE synergistically elicit ATP surge for surplus energy, autophagy for apoptotic evasion and chemo-resistance, insulin-like growth factor 1 (IGF-1) for meta-inflammation and angiogenesis, high mobility group box-1 (HMGB1) for immune tolerance, S100 proteins for metastasis, and p53 protein attenuation for tumour suppression. AGEs are pronouncedly reported in invasive forms of breast, prostate, colon and pancreatic cancers, higher in patients with cancer than healthy counterparts, and higher in advanced stage than localized phase. Hence, the investigation of person-specific presence of AGEs, soluble RAGE and AGE-activated RAGE can be advocated as impending bio-markers for diagnostic, prognostic and therapeutic purposes, to predict cancer risk in patients with diabetes, obesity, metabolic syndrome as well as general population, to monitor prognosis and metastasis in patients with cancer, and to reckon complications in cancer survivors. Furthermore, clinical reports of exogenous (dietary) and endogenous (internally formed) AGEs in cancer patients, and contemporary clinical trials involving AGE-RAGE axis in cancer are underlined with theranostic implications.
DOI: https://doi.org/10.37349/etat.2023.00170
This article belongs to the special issue Biomarkers for Personalized and Precise Cancer Diagnosis and Treatment
Despite consistent progress in prompt diagnosis and curative therapies in the last decade, lung cancer (LC) continues to threaten mankind, accounting for nearly twice the casualties compared to prostate, breast, and other cancers. Statistics associate ~25% of 2021 cancer-related deaths with LC, more than 80% of which are explicitly caused by tobacco smoking. Prevailing as small and non-small cell pathologies, with respective occurring frequency of nearly 15% and 80–85%, non-small cell LCs (NSCLCs) are prominently distinguished into lung adenocarcinoma (LUAD) and lung squamous cell carcinoma (LUSC), subtypes. Since the first use of epidermal growth factor receptor (EGFR) inhibitor gefitinib for NSCLC treatment in 2002, immense progress has been made for targeted therapies with the next generation of drugs spanning across the chronological generations of small molecule inhibitors. The last two years have overseen the clinical approval of more than 10 therapeutic agents as first-line NSCLC medications. However, uncertain mutational aberrations as well as systemic resistant responses, and abysmal overall survival curtail the combating efficacies. Of late, immune checkpoint inhibitors (ICIs) against various molecules including programmed cell death-1 (PD-1) and its ligand (PD-L1) have been demonstrated as reliable LC treatment targets. Keeping these aspects in mind, this review article discusses the success of NSCLC chemo and immunotherapies with their characteristic effectiveness and future perspectives.
Despite consistent progress in prompt diagnosis and curative therapies in the last decade, lung cancer (LC) continues to threaten mankind, accounting for nearly twice the casualties compared to prostate, breast, and other cancers. Statistics associate ~25% of 2021 cancer-related deaths with LC, more than 80% of which are explicitly caused by tobacco smoking. Prevailing as small and non-small cell pathologies, with respective occurring frequency of nearly 15% and 80–85%, non-small cell LCs (NSCLCs) are prominently distinguished into lung adenocarcinoma (LUAD) and lung squamous cell carcinoma (LUSC), subtypes. Since the first use of epidermal growth factor receptor (EGFR) inhibitor gefitinib for NSCLC treatment in 2002, immense progress has been made for targeted therapies with the next generation of drugs spanning across the chronological generations of small molecule inhibitors. The last two years have overseen the clinical approval of more than 10 therapeutic agents as first-line NSCLC medications. However, uncertain mutational aberrations as well as systemic resistant responses, and abysmal overall survival curtail the combating efficacies. Of late, immune checkpoint inhibitors (ICIs) against various molecules including programmed cell death-1 (PD-1) and its ligand (PD-L1) have been demonstrated as reliable LC treatment targets. Keeping these aspects in mind, this review article discusses the success of NSCLC chemo and immunotherapies with their characteristic effectiveness and future perspectives.
DOI: https://doi.org/10.37349/etat.2023.00171
This article belongs to the special issue Integrated Approaches for Non-Small-Cell Lung Cancer
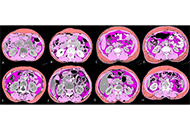
Aim:
Sarcopenia and skeletal muscle density (SMD) have been shown to be both predictive and prognostic marker in oncology. Advanced lung cancer inflammation index (ALI) has been shown to predict overall survival (OS) in small cell lung cancer (SCLC). Computed tomography (CT) enables skeletal muscle to be quantified, whereas body mass index (BMI) cannot accurately reflect body composition. The purpose was to evaluate the prognostic value of modified ALI (mALI) using CT-determined third lumbar vertebra (L3) muscle index beyond original ALI and see the interaction between sarcopenia, SMD, neutrophil-lymphocyte ratio (NLR), ALI and mALI at baseline and post 4 cycles of chemotherapy and their effects on OS and progress free survival (PFS) in patients with advanced non-SCLC (NSCLC).
Methods:
This retrospective study consisted of a total of 285 advanced NSCLC patients. The morphometric parameters such as SMD, skeletal muscle index (SMI) and fat-free mass (FFM) were measured by CT at the L3 vertebra. ALI was defined as BMI × serum albumin/NLR and mALI was defined as SMI × serum albumin/NLR.
Results:
Sarcopenia was observed in over 70% of patients across all BMI categories. Patients having sarcopenia suffered from a higher incidence of chemotherapeutic drug toxicities but this was not found to be statistically significant. Concordance was seen between ALI and mALI in the pre-treatment setting and this was statistically significant. A significant proportion of patients with poor ALI (90.9%), poor pre-chemotherapy mALI (91.3%) and poor post-chemotherapy mALI (89%) had poor NLR and each of them was statistically significant.
Conclusions:
In both univariate and multivariate analyses, this study demonstrated the statistical significance of sarcopenia, SMD, and mALI as predictive factors for OS. Additionally, sarcopenia and SMD were also found to be statistically significant factors in predicting PFS. These biomarkers could potentially help triage patients for active nutritional intervention for better outcomes.
Aim:
Sarcopenia and skeletal muscle density (SMD) have been shown to be both predictive and prognostic marker in oncology. Advanced lung cancer inflammation index (ALI) has been shown to predict overall survival (OS) in small cell lung cancer (SCLC). Computed tomography (CT) enables skeletal muscle to be quantified, whereas body mass index (BMI) cannot accurately reflect body composition. The purpose was to evaluate the prognostic value of modified ALI (mALI) using CT-determined third lumbar vertebra (L3) muscle index beyond original ALI and see the interaction between sarcopenia, SMD, neutrophil-lymphocyte ratio (NLR), ALI and mALI at baseline and post 4 cycles of chemotherapy and their effects on OS and progress free survival (PFS) in patients with advanced non-SCLC (NSCLC).
Methods:
This retrospective study consisted of a total of 285 advanced NSCLC patients. The morphometric parameters such as SMD, skeletal muscle index (SMI) and fat-free mass (FFM) were measured by CT at the L3 vertebra. ALI was defined as BMI × serum albumin/NLR and mALI was defined as SMI × serum albumin/NLR.
Results:
Sarcopenia was observed in over 70% of patients across all BMI categories. Patients having sarcopenia suffered from a higher incidence of chemotherapeutic drug toxicities but this was not found to be statistically significant. Concordance was seen between ALI and mALI in the pre-treatment setting and this was statistically significant. A significant proportion of patients with poor ALI (90.9%), poor pre-chemotherapy mALI (91.3%) and poor post-chemotherapy mALI (89%) had poor NLR and each of them was statistically significant.
Conclusions:
In both univariate and multivariate analyses, this study demonstrated the statistical significance of sarcopenia, SMD, and mALI as predictive factors for OS. Additionally, sarcopenia and SMD were also found to be statistically significant factors in predicting PFS. These biomarkers could potentially help triage patients for active nutritional intervention for better outcomes.
DOI: https://doi.org/10.37349/etat.2023.00172
This article belongs to the special issue Biomarkers for Personalized and Precise Cancer Diagnosis and Treatment
Breast cancer (BC) is a leading cause of cancer-related deaths in women worldwide where the process of metastasis is a major contributor to the mortality associated with this disease. Metastasis suppressor genes are a group of genes that play a crucial role in preventing or inhibiting the spread of cancer cells. They suppress the metastasis process by inhibiting colonization and by inducing dormancy. These genes function by regulating various cellular processes in the tumor microenvironment (TME), such as cell adhesion, invasion, migration, and angiogenesis. Dysregulation of metastasis suppressor genes can lead to the acquisition of an invasive and metastatic phenotype and lead to poor prognostic outcomes. The components of the TME generally play a necessary in the metastasis progression of tumor cells. This review has identified and elaborated on the role of a few metastatic suppressors associated with the TME that have been shown to inhibit metastasis in BC by different mechanisms, such as blocking certain cell signaling molecules involved in cancer cell migration, invasion, enhancing immune surveillance of cancer cells, and promoting the formation of a protective extracellular matrix (ECM). Understanding the interaction of metastatic suppressor genes and the components of TME has important implications for the development of novel therapeutic strategies to target the metastatic cascade. Targeting these genes or their downstream signaling pathways offers a promising approach to inhibiting the spread of cancer cells and improves patient outcomes.
Breast cancer (BC) is a leading cause of cancer-related deaths in women worldwide where the process of metastasis is a major contributor to the mortality associated with this disease. Metastasis suppressor genes are a group of genes that play a crucial role in preventing or inhibiting the spread of cancer cells. They suppress the metastasis process by inhibiting colonization and by inducing dormancy. These genes function by regulating various cellular processes in the tumor microenvironment (TME), such as cell adhesion, invasion, migration, and angiogenesis. Dysregulation of metastasis suppressor genes can lead to the acquisition of an invasive and metastatic phenotype and lead to poor prognostic outcomes. The components of the TME generally play a necessary in the metastasis progression of tumor cells. This review has identified and elaborated on the role of a few metastatic suppressors associated with the TME that have been shown to inhibit metastasis in BC by different mechanisms, such as blocking certain cell signaling molecules involved in cancer cell migration, invasion, enhancing immune surveillance of cancer cells, and promoting the formation of a protective extracellular matrix (ECM). Understanding the interaction of metastatic suppressor genes and the components of TME has important implications for the development of novel therapeutic strategies to target the metastatic cascade. Targeting these genes or their downstream signaling pathways offers a promising approach to inhibiting the spread of cancer cells and improves patient outcomes.
DOI: https://doi.org/10.37349/etat.2023.00173
This article belongs to the special issue Therapeutic Targeting of the Tumor Microenvironment
Aim:
Artificial intelligence (AI) is a new field of science in which computers will provide decisions-supporting tools to help doctors make difficult clinical choices. Recent AI applications in otolaryngology include head and neck oncology, rhinology, neurotology, and laryngology. The aim of this systematic review is to describe the potential uses of AI in head and neck oncology with a special focus on the surgical field.
Methods:
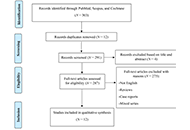
The authors performed a systematic review, in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, in the main medical databases, including PubMed, Scopus, and Cochrane Library, considering all original studies published until February 2023 about the role of AI in head and neck cancer surgery. The search strategy included a combination of the following terms: “artificial intelligence” or “machine learning” and “head and neck cancer”.
Results:
Overall, 303 papers were identified and after duplicate removal (12 papers) and excluding papers not written in English (1 paper) and off-topic (4 papers), papers were assessed for eligibility; finally, only 12 papers were included. Three main fields of clinical interest were identified: the most widely investigated included the role of AI in surgical margins assessment (7 papers); the second most frequently evaluated topic was complications assessment (4 papers); finally, only one paper dealt with the indication of salvage laryngectomy after primary radiotherapy.
Conclusions:
The authors report the first systematic review in the literature concerning the role of AI in head and neck cancer surgery. An increasing influx of AI applications to clinical problems in otolaryngology is expected, so specialists should be increasingly prepared to manage the constant changes. It will always remain critical for clinicians to use their skills and knowledge to critically evaluate the additional information provided by AI and make the final decisions on each patient.
Aim:
Artificial intelligence (AI) is a new field of science in which computers will provide decisions-supporting tools to help doctors make difficult clinical choices. Recent AI applications in otolaryngology include head and neck oncology, rhinology, neurotology, and laryngology. The aim of this systematic review is to describe the potential uses of AI in head and neck oncology with a special focus on the surgical field.
Methods:
The authors performed a systematic review, in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, in the main medical databases, including PubMed, Scopus, and Cochrane Library, considering all original studies published until February 2023 about the role of AI in head and neck cancer surgery. The search strategy included a combination of the following terms: “artificial intelligence” or “machine learning” and “head and neck cancer”.
Results:
Overall, 303 papers were identified and after duplicate removal (12 papers) and excluding papers not written in English (1 paper) and off-topic (4 papers), papers were assessed for eligibility; finally, only 12 papers were included. Three main fields of clinical interest were identified: the most widely investigated included the role of AI in surgical margins assessment (7 papers); the second most frequently evaluated topic was complications assessment (4 papers); finally, only one paper dealt with the indication of salvage laryngectomy after primary radiotherapy.
Conclusions:
The authors report the first systematic review in the literature concerning the role of AI in head and neck cancer surgery. An increasing influx of AI applications to clinical problems in otolaryngology is expected, so specialists should be increasingly prepared to manage the constant changes. It will always remain critical for clinicians to use their skills and knowledge to critically evaluate the additional information provided by AI and make the final decisions on each patient.
DOI: https://doi.org/10.37349/etat.2023.00174
This article belongs to the special issue Artificial Intelligence for Precision Oncology
Renal cell carcinoma (RCC) is one of the most life-threatening urinary malignancies displaying poor response to radiotherapy and chemotherapy. Although in the recent past there have been tremendous advancements in using targeted therapies for RCC, despite that it remains the most lethal urogenital cancer with a 5-year survival rate of roughly 76%. Timely diagnosis is still the key to prevent the progression of RCC into metastatic stages as well as to treat it. But due to the lack of definitive and specific diagnostic biomarkers for RCC and its asymptomatic nature in its early stages, it becomes very difficult to diagnose it. Reliable and distinct molecular markers can not only refine the diagnosis but also classifies the tumors into thier sub-types which can escort subsequent management and possible treatment for patients. Potential biomarkers can permit a greater degree of stratification of patients affected by RCC and help tailor novel targeted therapies. The review summarizes the most promising epigenetic [DNA methylation, microRNA (miRNA; miR), and long noncoding RNA (lncRNA)] and protein biomarkers that have been known to be specifically involved in diagnosis, cancer progression, and metastasis of RCC, thereby highlighting their utilization as non-invasive molecular markers in RCC. Also, the rationale and development of novel molecular targeted drugs and immunotherapy drugs [such as tyrosine kinase inhibitors and immune checkpoint inhibitors (ICIs)] as potential RCC therapeutics along with the proposed implication of these biomarkers in predicting response to targeted therapies will be discussed.
Renal cell carcinoma (RCC) is one of the most life-threatening urinary malignancies displaying poor response to radiotherapy and chemotherapy. Although in the recent past there have been tremendous advancements in using targeted therapies for RCC, despite that it remains the most lethal urogenital cancer with a 5-year survival rate of roughly 76%. Timely diagnosis is still the key to prevent the progression of RCC into metastatic stages as well as to treat it. But due to the lack of definitive and specific diagnostic biomarkers for RCC and its asymptomatic nature in its early stages, it becomes very difficult to diagnose it. Reliable and distinct molecular markers can not only refine the diagnosis but also classifies the tumors into thier sub-types which can escort subsequent management and possible treatment for patients. Potential biomarkers can permit a greater degree of stratification of patients affected by RCC and help tailor novel targeted therapies. The review summarizes the most promising epigenetic [DNA methylation, microRNA (miRNA; miR), and long noncoding RNA (lncRNA)] and protein biomarkers that have been known to be specifically involved in diagnosis, cancer progression, and metastasis of RCC, thereby highlighting their utilization as non-invasive molecular markers in RCC. Also, the rationale and development of novel molecular targeted drugs and immunotherapy drugs [such as tyrosine kinase inhibitors and immune checkpoint inhibitors (ICIs)] as potential RCC therapeutics along with the proposed implication of these biomarkers in predicting response to targeted therapies will be discussed.
DOI: https://doi.org/10.37349/etat.2023.00175
This article belongs to the special issue Biomarkers for Personalized and Precise Cancer Diagnosis and Treatment
A dysregulated circadian rhythm is significantly associated with cancer risk, as is aging. Both aging and circadian dysregulation show suppressed pineal melatonin, which is indicated in many studies to be linked to cancer risk and progression. Another independently investigated aspect of the circadian rhythm is the cortisol awakening response (CAR), which is linked to stress-associated hypothalamus-pituitary-adrenal (HPA) axis activation. CAR and HPA axis activity are primarily mediated via activation of the glucocorticoid receptor (GR), which drives patterned gene expression via binding to the promotors of glucocorticoid response element (GRE)-expressing genes. Recent data shows that the GR can be prevented from nuclear translocation by the B cell lymphoma-2 (Bcl-2)-associated athanogene 1 (BAG-1), which translocates the GR to mitochondria, where it can have diverse effects. Melatonin also suppresses GR nuclear translocation by maintaining the GR in a complex with heat shock protein 90 (Hsp90). Melatonin, directly and/or epigenetically, can upregulate BAG-1, suggesting that the dramatic 10-fold decrease in pineal melatonin from adolescence to the ninth decade of life will attenuate the capacity of night-time melatonin to modulate the effects of the early morning CAR. The interactions of pineal melatonin/BAG-1/Hsp90 with the CAR are proposed to underpin how aging and circadian dysregulation are associated with cancer risk. This may be mediated via differential effects of melatonin/BAG-1/Hsp90/GR in different cells of microenvironments across the body, from which tumors emerge. This provides a model of cancer pathogenesis that better integrates previously disparate bodies of data, including how immune cells are regulated by cancer cells in the tumor microenvironment, at least partly via the cancer cell regulation of the tryptophan-melatonin pathway. This has a number of future research and treatment implications.
A dysregulated circadian rhythm is significantly associated with cancer risk, as is aging. Both aging and circadian dysregulation show suppressed pineal melatonin, which is indicated in many studies to be linked to cancer risk and progression. Another independently investigated aspect of the circadian rhythm is the cortisol awakening response (CAR), which is linked to stress-associated hypothalamus-pituitary-adrenal (HPA) axis activation. CAR and HPA axis activity are primarily mediated via activation of the glucocorticoid receptor (GR), which drives patterned gene expression via binding to the promotors of glucocorticoid response element (GRE)-expressing genes. Recent data shows that the GR can be prevented from nuclear translocation by the B cell lymphoma-2 (Bcl-2)-associated athanogene 1 (BAG-1), which translocates the GR to mitochondria, where it can have diverse effects. Melatonin also suppresses GR nuclear translocation by maintaining the GR in a complex with heat shock protein 90 (Hsp90). Melatonin, directly and/or epigenetically, can upregulate BAG-1, suggesting that the dramatic 10-fold decrease in pineal melatonin from adolescence to the ninth decade of life will attenuate the capacity of night-time melatonin to modulate the effects of the early morning CAR. The interactions of pineal melatonin/BAG-1/Hsp90 with the CAR are proposed to underpin how aging and circadian dysregulation are associated with cancer risk. This may be mediated via differential effects of melatonin/BAG-1/Hsp90/GR in different cells of microenvironments across the body, from which tumors emerge. This provides a model of cancer pathogenesis that better integrates previously disparate bodies of data, including how immune cells are regulated by cancer cells in the tumor microenvironment, at least partly via the cancer cell regulation of the tryptophan-melatonin pathway. This has a number of future research and treatment implications.
DOI: https://doi.org/10.37349/etat.2023.00176
This article belongs to the special issue Novel Insights into Immunotherapy Targeting Tumor Microenvironment in Cancer
The present coronavirus disease 2019 (COVID-19) pandemic scenario has posed a difficulty for cancer treatment. Even under ideal conditions, malignancies like small cell lung cancer (SCLC) are challenging to treat because of their fast development and early metastases. The treatment of these patients must not be jeopardized, and they must be protected as much as possible from the continuous spread of the COVID-19 infection. Initially identified in December 2019 in Wuhan, China, the contagious coronavirus illness 2019 (COVID-19) is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Finding inhibitors against the druggable targets of SARS-CoV-2 has been a significant focus of research efforts across the globe. The primary motivation for using molecular modeling tools against SARS-CoV-2 was to identify candidates for use as therapeutic targets from a pharmacological database. In the published study, scientists used a combination of medication repurposing and virtual drug screening methodologies to target many structures of SARS-CoV-2. This virus plays an essential part in the maturation and replication of other viruses. In addition, the total binding free energy and molecular dynamics (MD) modeling findings showed that the dynamics of various medications and substances were stable; some of them have been tested experimentally against SARS-CoV-2. Different virtual screening (VS) methods have been discussed as potential means by which the evaluated medications that show strong binding to the active site might be repurposed for use against SARS-CoV-2.
The present coronavirus disease 2019 (COVID-19) pandemic scenario has posed a difficulty for cancer treatment. Even under ideal conditions, malignancies like small cell lung cancer (SCLC) are challenging to treat because of their fast development and early metastases. The treatment of these patients must not be jeopardized, and they must be protected as much as possible from the continuous spread of the COVID-19 infection. Initially identified in December 2019 in Wuhan, China, the contagious coronavirus illness 2019 (COVID-19) is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Finding inhibitors against the druggable targets of SARS-CoV-2 has been a significant focus of research efforts across the globe. The primary motivation for using molecular modeling tools against SARS-CoV-2 was to identify candidates for use as therapeutic targets from a pharmacological database. In the published study, scientists used a combination of medication repurposing and virtual drug screening methodologies to target many structures of SARS-CoV-2. This virus plays an essential part in the maturation and replication of other viruses. In addition, the total binding free energy and molecular dynamics (MD) modeling findings showed that the dynamics of various medications and substances were stable; some of them have been tested experimentally against SARS-CoV-2. Different virtual screening (VS) methods have been discussed as potential means by which the evaluated medications that show strong binding to the active site might be repurposed for use against SARS-CoV-2.
DOI: https://doi.org/10.37349/etat.2023.00177
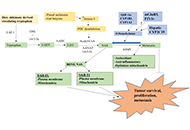
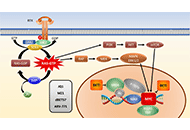
Mutant Kirsten rat sarcoma viral oncogene homolog (KRAS) is now a drugable oncogenic driver and the KRAS G12C variant responds clinically to sotorasib and adagrasib that covalently block the cysteine of the active center and inhibit downstream signaling and proliferation. Unfortunately, progression-free survival (PFS) of lung cancer patients is only 5–6 months and no survival advantage has been found for sotorasib in comparison to docetaxel chemotherapy. Increased responses to KRAS inhibitors are tested in combination with the son of sevenless 1 (SOS1) inhibitors, upstream and downstream signaling modulators as well as chemotherapeutics. Some of these approaches are limited by toxicity to normal tissues and by diverse mechanisms of resistance. In essence, most of these attempts are directed to the inhibition of proliferation by impairment of the signal transduction pathways. The final target of KRAS-mediated growth stimulation is MYC in the cell nucleus that stimulates transcription of a host of genes. In detail, MYC alters genomic enhancer and super-enhancers of transcription that are frequently deregulated in cancer. Such enhancers can be targeted by bromodomain and extra-terminal (BET) inhibitors (BETi) or degraders and this review discusses whether integrated SOS1 inhibition and BET targeting of MYC synergizes against mutant KRAS tumor growth. BET degraders in the form of proteolysis-targeting chimeras (PROTACs) combined with BAY-293-mediated SOS1 inhibition revealed marked cytotoxic synergy against mutant KRAS cancer cells and may constitute a promising option for clinical treatment.
Mutant Kirsten rat sarcoma viral oncogene homolog (KRAS) is now a drugable oncogenic driver and the KRAS G12C variant responds clinically to sotorasib and adagrasib that covalently block the cysteine of the active center and inhibit downstream signaling and proliferation. Unfortunately, progression-free survival (PFS) of lung cancer patients is only 5–6 months and no survival advantage has been found for sotorasib in comparison to docetaxel chemotherapy. Increased responses to KRAS inhibitors are tested in combination with the son of sevenless 1 (SOS1) inhibitors, upstream and downstream signaling modulators as well as chemotherapeutics. Some of these approaches are limited by toxicity to normal tissues and by diverse mechanisms of resistance. In essence, most of these attempts are directed to the inhibition of proliferation by impairment of the signal transduction pathways. The final target of KRAS-mediated growth stimulation is MYC in the cell nucleus that stimulates transcription of a host of genes. In detail, MYC alters genomic enhancer and super-enhancers of transcription that are frequently deregulated in cancer. Such enhancers can be targeted by bromodomain and extra-terminal (BET) inhibitors (BETi) or degraders and this review discusses whether integrated SOS1 inhibition and BET targeting of MYC synergizes against mutant KRAS tumor growth. BET degraders in the form of proteolysis-targeting chimeras (PROTACs) combined with BAY-293-mediated SOS1 inhibition revealed marked cytotoxic synergy against mutant KRAS cancer cells and may constitute a promising option for clinical treatment.
DOI: https://doi.org/10.37349/etat.2023.00178
This article belongs to the special issue Integrated Approaches for Non-Small-Cell Lung Cancer
