














Metabolic dysfunction-associated steatotic liver disease (MASLD) is increasingly recognized as a multisystem disorder in which iron acts as both a metabolic “spark” and an accelerant of liver injury. This integrates emerging evidence that iron-driven oxidative stress and low-grade inflammation are mutually reinforcing processes in metabolic liver disease. In this perspective article, epidemiological evidence, molecular insights, and emerging clinical data are integrated to clarify how hyperferritinemia, often dismissed as a mere inflammatory marker, maps onto genuine iron redistribution and overload in the metabolic liver. Physiological iron homeostasis and its disruption by adiposity-related inflammation, hyperinsulinemia, sex hormones, and common HFE variants, creating a labile catalytic iron pool that fuels Fenton chemistry in lipid-laden hepatocytes. Population studies and expert-panel criteria are summarized that define “metabolic hyperferritinemia” and stratify dysmetabolic iron accumulation into three magnetic resonance imaging (MRI)-based grades, each linked to stepwise increases in steatosis, fibrosis, and clinical events. Mechanistically, excess Fe2+ triggers lipid peroxidation, mitochondrial dysfunction, ferroptosis, Kupffer cell activation, endoplasmic reticulum stress, and hepatic stellate cell sensitization to TGF-β, thereby accelerating the transition from steatosis to steatohepatitis and fibrosis. Finally, the diagnostic algorithms, iron-modulating therapies (phlebotomy, hepcidin agonists, diet), and prospective data supporting ferritin-based triage in clinics are discussed. Collectively, the outlined evidence positions iron not only as a biomarker but also as a modifiable driver of MASLD progression, underscoring the need for randomized trials that test whether targeted iron reduction improves hard hepatic outcomes.
Metabolic dysfunction-associated steatotic liver disease (MASLD) is increasingly recognized as a multisystem disorder in which iron acts as both a metabolic “spark” and an accelerant of liver injury. This integrates emerging evidence that iron-driven oxidative stress and low-grade inflammation are mutually reinforcing processes in metabolic liver disease. In this perspective article, epidemiological evidence, molecular insights, and emerging clinical data are integrated to clarify how hyperferritinemia, often dismissed as a mere inflammatory marker, maps onto genuine iron redistribution and overload in the metabolic liver. Physiological iron homeostasis and its disruption by adiposity-related inflammation, hyperinsulinemia, sex hormones, and common HFE variants, creating a labile catalytic iron pool that fuels Fenton chemistry in lipid-laden hepatocytes. Population studies and expert-panel criteria are summarized that define “metabolic hyperferritinemia” and stratify dysmetabolic iron accumulation into three magnetic resonance imaging (MRI)-based grades, each linked to stepwise increases in steatosis, fibrosis, and clinical events. Mechanistically, excess Fe2+ triggers lipid peroxidation, mitochondrial dysfunction, ferroptosis, Kupffer cell activation, endoplasmic reticulum stress, and hepatic stellate cell sensitization to TGF-β, thereby accelerating the transition from steatosis to steatohepatitis and fibrosis. Finally, the diagnostic algorithms, iron-modulating therapies (phlebotomy, hepcidin agonists, diet), and prospective data supporting ferritin-based triage in clinics are discussed. Collectively, the outlined evidence positions iron not only as a biomarker but also as a modifiable driver of MASLD progression, underscoring the need for randomized trials that test whether targeted iron reduction improves hard hepatic outcomes.
DOI: https://doi.org/10.37349/edd.2025.100599
This article belongs to the special issue Advances in Hepato-gastroenterology: Diagnosis, Prognostication, and Disease Stratification
Aim:
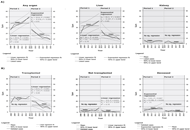
In Switzerland, the first access to interferon-free direct-acting antivirals (DAAs) for hepatitis C virus (HCV) treatment was in 2014. This study aimed to analyze the effects of DAAs on the yearly listed numbers of HCV RNA-positive (RNA+) patients and their mortality on the Swiss organ transplantation waiting list (SOWL).
Methods:
In this retrospective secondary time series analysis of yearly aggregated data on listed and delisted patients from a subset of HCV RNA+ patients on the SOWL, listed patients were grouped by the requested organ, and delisted patients by reason. Time series were split into two periods of equal length, the phases before and after DAA implementation, and the mean difference was tested using the Mann-Whitney U test.
Results:
From 2008 to 2019, 328 HCV RNA+ patients were listed on SOWL, 86.6% requesting liver, 11.6% kidney, and 1.8% other organ transplantations. A total of 285 RNA+ patients were delisted from SOWL: 14.7% died, 75.4% had been transplanted, and 9.8% were delisted without surgery. There were significant reductions of patients listed for requesting any organ (–21.7, P = 0.004), liver (–18.3, P = 0.004), or kidney (–3.0, P = 0.031) comparing the periods before and after DAA launch. The mean number of delistings after transplantation (–11.2, P = 0.010), or death (–4, P < 0.001) show a significant reduction.
Conclusions:
With DAAs, the rising trend of HCV RNA+ people waiting for organs was broken, as was the increasing trend of mortality on the SOWL among HCV RNA+ individuals.
Aim:
In Switzerland, the first access to interferon-free direct-acting antivirals (DAAs) for hepatitis C virus (HCV) treatment was in 2014. This study aimed to analyze the effects of DAAs on the yearly listed numbers of HCV RNA-positive (RNA+) patients and their mortality on the Swiss organ transplantation waiting list (SOWL).
Methods:
In this retrospective secondary time series analysis of yearly aggregated data on listed and delisted patients from a subset of HCV RNA+ patients on the SOWL, listed patients were grouped by the requested organ, and delisted patients by reason. Time series were split into two periods of equal length, the phases before and after DAA implementation, and the mean difference was tested using the Mann-Whitney U test.
Results:
From 2008 to 2019, 328 HCV RNA+ patients were listed on SOWL, 86.6% requesting liver, 11.6% kidney, and 1.8% other organ transplantations. A total of 285 RNA+ patients were delisted from SOWL: 14.7% died, 75.4% had been transplanted, and 9.8% were delisted without surgery. There were significant reductions of patients listed for requesting any organ (–21.7, P = 0.004), liver (–18.3, P = 0.004), or kidney (–3.0, P = 0.031) comparing the periods before and after DAA launch. The mean number of delistings after transplantation (–11.2, P = 0.010), or death (–4, P < 0.001) show a significant reduction.
Conclusions:
With DAAs, the rising trend of HCV RNA+ people waiting for organs was broken, as was the increasing trend of mortality on the SOWL among HCV RNA+ individuals.
DOI: https://doi.org/10.37349/edd.2023.00032
DOI: https://doi.org/10.37349/edd.2024.00035
DOI: https://doi.org/10.37349/edd.2024.00036
This article belongs to the special issue Latest Updates in the Endoscopic, Surgical and Medical Treatment of Resectable and Advanced Gastrointestinal Cancers
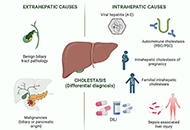
Drug-induced liver injury (DILI) is an adverse reaction to drugs and other xenobiotics that can have serious consequences and jeopardise progress in pharmacological therapy. While DILI is predominantly hepatocellular, a non-negligible percentage of patients who present with cholestatic damage. Mixed damage is typically lumped together with cholestatic damage in the literature. Drug-induced cholestasis is often caused by the use of some non-steroidal anti-inflammatory drugs (NSAIDs), antibiotics (i.e., amoxicillin-clavulanic acid), statins, and anabolic agents, among others. Drug-associated cholestasis tends to have a more chronic course and mostly affects older population. There is also a genetic predisposition to toxic cholestasis caused by some drugs (amoxicillin-clavulanic acid, statins, etc.). Recently, anatomical alterations of the biliary tract induced by drugs (especially immunotherapy drugs) have been described. Bile duct injury is one of the histopathological findings that have prognostic significance in DILI. A correct differential diagnosis with other causes of cholestasis is mandatory to reach an accurate diagnosis. Ursodexycholic acid, corticosteroids, and replacement therapies have been used as a therapeutic arsenal, although more evidence is needed to establish them as a routine therapeutic management in clinical practice. The breakthrough and validation of biomarkers of cholestasis and bile duct injury is an urgent need for drug development and post-marketing phase.
Drug-induced liver injury (DILI) is an adverse reaction to drugs and other xenobiotics that can have serious consequences and jeopardise progress in pharmacological therapy. While DILI is predominantly hepatocellular, a non-negligible percentage of patients who present with cholestatic damage. Mixed damage is typically lumped together with cholestatic damage in the literature. Drug-induced cholestasis is often caused by the use of some non-steroidal anti-inflammatory drugs (NSAIDs), antibiotics (i.e., amoxicillin-clavulanic acid), statins, and anabolic agents, among others. Drug-associated cholestasis tends to have a more chronic course and mostly affects older population. There is also a genetic predisposition to toxic cholestasis caused by some drugs (amoxicillin-clavulanic acid, statins, etc.). Recently, anatomical alterations of the biliary tract induced by drugs (especially immunotherapy drugs) have been described. Bile duct injury is one of the histopathological findings that have prognostic significance in DILI. A correct differential diagnosis with other causes of cholestasis is mandatory to reach an accurate diagnosis. Ursodexycholic acid, corticosteroids, and replacement therapies have been used as a therapeutic arsenal, although more evidence is needed to establish them as a routine therapeutic management in clinical practice. The breakthrough and validation of biomarkers of cholestasis and bile duct injury is an urgent need for drug development and post-marketing phase.
DOI: https://doi.org/10.37349/edd.2023.00027
This article belongs to the special issue CHOLESTASIS
The pathogenesis of primary biliary cholangitis (PBC) is particularly complicated as both intrinsic and extrinsic factors are implicated. Several forms of cellular death, both programmable and non-programmable, operate leading biliary epithelial cells (BECs) to elimination. The precise role of critical pathways like autophagy, apoptosis, senescence, and their interplay has not been fully clarified. Therefore, in this review, data on these important mechanisms are presented and their implication in PBC is discussed. The interplay of the three mechanisms is examined and the factors that drive them are analyzed. Moreover, the upstream drivers of autophagy, apoptosis, and senescence are presented. They include the loss of the protective bicarbonate umbrella in BECs due to the reduction of activity of the anion exchanger 2 (AE2) with the resultant activation of the intracellular soluble adenylyl cyclase (sAC). The role of toxic bile acids is also presented. A sequence of events is proposed including involvement of the gut-liver axis and the possible role of ferroptosis. Finally, a brief account of the initial trigger of the disease is given.
The pathogenesis of primary biliary cholangitis (PBC) is particularly complicated as both intrinsic and extrinsic factors are implicated. Several forms of cellular death, both programmable and non-programmable, operate leading biliary epithelial cells (BECs) to elimination. The precise role of critical pathways like autophagy, apoptosis, senescence, and their interplay has not been fully clarified. Therefore, in this review, data on these important mechanisms are presented and their implication in PBC is discussed. The interplay of the three mechanisms is examined and the factors that drive them are analyzed. Moreover, the upstream drivers of autophagy, apoptosis, and senescence are presented. They include the loss of the protective bicarbonate umbrella in BECs due to the reduction of activity of the anion exchanger 2 (AE2) with the resultant activation of the intracellular soluble adenylyl cyclase (sAC). The role of toxic bile acids is also presented. A sequence of events is proposed including involvement of the gut-liver axis and the possible role of ferroptosis. Finally, a brief account of the initial trigger of the disease is given.
DOI: https://doi.org/10.37349/edd.2023.00028
This article belongs to the special issue CHOLESTASIS
Non-alcoholic fatty liver disease (NAFLD) is the leading chronic liver disease worldwide, with a progressive form of non-alcoholic steatohepatitis (NASH). It may progress to advanced liver diseases, including liver fibrosis, cirrhosis, and hepatocellular carcinoma. NAFLD/NASH is a comorbidity of many metabolic disorders such as obesity, insulin resistance, type 2 diabetes, cardiovascular disease, and chronic kidney disease. These metabolic diseases are often accompanied by systemic or extrahepatic inflammation, which plays an important role in the pathogenesis and treatment of NAFLD or NASH. Metabolites, such as short-chain fatty acids, impact the function, inflammation, and death of hepatocytes, the primary parenchymal cells in the liver tissue. Cholangiocytes, the epithelial cells that line the bile ducts, can differentiate into proliferative hepatocytes in chronic liver injury. In addition, hepatic non-parenchymal cells, including liver sinusoidal endothelial cells, hepatic stellate cells, and innate and adaptive immune cells, are involved in liver inflammation. Proteins such as fibroblast growth factors, acetyl-coenzyme A carboxylases, and nuclear factor erythroid 2-related factor 2 are involved in liver metabolism and inflammation, which are potential targets for NASH treatment. This review focuses on the effects of metabolic disease-induced extrahepatic inflammation, liver inflammation, and the cellular and molecular mechanisms of liver metabolism on the development and progression of NAFLD and NASH, as well as the associated treatments.
Non-alcoholic fatty liver disease (NAFLD) is the leading chronic liver disease worldwide, with a progressive form of non-alcoholic steatohepatitis (NASH). It may progress to advanced liver diseases, including liver fibrosis, cirrhosis, and hepatocellular carcinoma. NAFLD/NASH is a comorbidity of many metabolic disorders such as obesity, insulin resistance, type 2 diabetes, cardiovascular disease, and chronic kidney disease. These metabolic diseases are often accompanied by systemic or extrahepatic inflammation, which plays an important role in the pathogenesis and treatment of NAFLD or NASH. Metabolites, such as short-chain fatty acids, impact the function, inflammation, and death of hepatocytes, the primary parenchymal cells in the liver tissue. Cholangiocytes, the epithelial cells that line the bile ducts, can differentiate into proliferative hepatocytes in chronic liver injury. In addition, hepatic non-parenchymal cells, including liver sinusoidal endothelial cells, hepatic stellate cells, and innate and adaptive immune cells, are involved in liver inflammation. Proteins such as fibroblast growth factors, acetyl-coenzyme A carboxylases, and nuclear factor erythroid 2-related factor 2 are involved in liver metabolism and inflammation, which are potential targets for NASH treatment. This review focuses on the effects of metabolic disease-induced extrahepatic inflammation, liver inflammation, and the cellular and molecular mechanisms of liver metabolism on the development and progression of NAFLD and NASH, as well as the associated treatments.
DOI: https://doi.org/10.37349/edd.2023.00029
Aim:
Familial achalasia (FA) is a very rare condition. This work aims to evaluate its prevalence, characterize its clinical profile in a large series, and assess the efficacy and safety of pneumatic dilation (PD) in this context.
Methods:
A total of 817 patients with achalasia were collected over a period of 20 years (1990–2010). All cases of FA: isolated or associated to Allgrove syndrome, were looked for in both parents and siblings.
Results:
In this study, 18 families with FA were identified n = 41 patients (5%). Two members were affected in each family, in 14 families, three members per family in three others, and for the remaining family 04 members. All cases of achalasia were observed in siblings and parent to child transmission was unfound. Achalasia was associated to Allgrove syndrome in 15 families. It was isolated in 3 families. Consanguinity was found in 89% of patients, and death at a young age in the siblings was recorded in 27% of cases. Achalasia was present before the age of 5 years in 75% of cases. There was no difference between the two groups for age, age at onset, sex and the presence of the cardinal signs of achalasia. A total of 102 dilations were performed. Only one session in 31% of cases, two in 38%, three in 17% and more than three sessions in 14%. The long-term success rate of PD was low.
Conclusions:
FA manifests almost exclusively in childhood. It is rarely isolated; most often falls under Allgrove syndrome. Alacrima is the earliest sign that should lead to the diagnosis. The long-term success rate of PD is rather low. This requires recourse to multiple sessions of PD or Heller’s cardiomyotomy which may be the best initial approach.
Aim:
Familial achalasia (FA) is a very rare condition. This work aims to evaluate its prevalence, characterize its clinical profile in a large series, and assess the efficacy and safety of pneumatic dilation (PD) in this context.
Methods:
A total of 817 patients with achalasia were collected over a period of 20 years (1990–2010). All cases of FA: isolated or associated to Allgrove syndrome, were looked for in both parents and siblings.
Results:
In this study, 18 families with FA were identified n = 41 patients (5%). Two members were affected in each family, in 14 families, three members per family in three others, and for the remaining family 04 members. All cases of achalasia were observed in siblings and parent to child transmission was unfound. Achalasia was associated to Allgrove syndrome in 15 families. It was isolated in 3 families. Consanguinity was found in 89% of patients, and death at a young age in the siblings was recorded in 27% of cases. Achalasia was present before the age of 5 years in 75% of cases. There was no difference between the two groups for age, age at onset, sex and the presence of the cardinal signs of achalasia. A total of 102 dilations were performed. Only one session in 31% of cases, two in 38%, three in 17% and more than three sessions in 14%. The long-term success rate of PD was low.
Conclusions:
FA manifests almost exclusively in childhood. It is rarely isolated; most often falls under Allgrove syndrome. Alacrima is the earliest sign that should lead to the diagnosis. The long-term success rate of PD is rather low. This requires recourse to multiple sessions of PD or Heller’s cardiomyotomy which may be the best initial approach.
DOI: https://doi.org/10.37349/edd.2023.00030
This article belongs to the special issue Advances in Hepato-gastroenterology: Diagnosis, Prognostication, and Disease Stratification
DOI: https://doi.org/10.37349/edd.2022.00001
The prevalence of metabolic dysfunction-associated fatty liver disease (MAFLD) is increasing rapidly worldwide due to the obesity epidemic. Advanced stages of the MAFLD, such as non-alcoholic steatohepatitis (NASH) with advanced fibrosis or cirrhosis are affecting global health. Extracellular vesicles (EVs) are released by all cell types and are important in cell-to-cell communication and maintaining homeostasis, but they also play a role in the pathogenesis of various diseases. EVs contain biological information such as lipids, proteins, messenger RNAs (mRNAs), small RNAs, and DNA, and they act on (distant) target cells. The cargo of EVs is dependent on the type and the state of the releasing cell. EVs have been proposed as biomarkers, prognostic, and even therapeutic agents, also in the context of liver diseases. This review aims to give an overview of the current knowledge on EVs in MAFLD, including the role and interaction of EVs with different cell types in the liver. Several aspects of EVs, including their origin, characteristics, cargo, and functions are reviewed. Moreover, the potential of EVs as targets for the treatment of MAFLD is discussed.
The prevalence of metabolic dysfunction-associated fatty liver disease (MAFLD) is increasing rapidly worldwide due to the obesity epidemic. Advanced stages of the MAFLD, such as non-alcoholic steatohepatitis (NASH) with advanced fibrosis or cirrhosis are affecting global health. Extracellular vesicles (EVs) are released by all cell types and are important in cell-to-cell communication and maintaining homeostasis, but they also play a role in the pathogenesis of various diseases. EVs contain biological information such as lipids, proteins, messenger RNAs (mRNAs), small RNAs, and DNA, and they act on (distant) target cells. The cargo of EVs is dependent on the type and the state of the releasing cell. EVs have been proposed as biomarkers, prognostic, and even therapeutic agents, also in the context of liver diseases. This review aims to give an overview of the current knowledge on EVs in MAFLD, including the role and interaction of EVs with different cell types in the liver. Several aspects of EVs, including their origin, characteristics, cargo, and functions are reviewed. Moreover, the potential of EVs as targets for the treatment of MAFLD is discussed.
DOI: https://doi.org/10.37349/edd.2022.00002
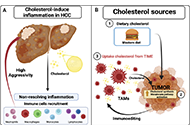
Hepatocellular carcinoma (HCC) is considered one of the most aggressive tumors worldwide. The consumption of lipid-enriched diets, mainly high cholesterol, induces oxidative stress and chronic inflammation, leading to HCC progression. Moreover, fatty acids and cholesterol could display differential responses on immune cells inside the tumor immune microenvironment (TIME). Tumor-associated macrophages (TAMs) represent one of the most critical leukocytes in the tumor microenvironment (TME) displaying pro-tumoral responses and one of the mainly cholesterol donors to cancer cells. Immunotherapy or cholesterol regulators, alone or combined, would represent an effective strategy for HCC treatment. Nonetheless, steatotic etiology from non-alcoholic fatty liver disease (NAFLD)-HCC tumors has been unexpectedly resulting in highly aggressive behavior.
Hepatocellular carcinoma (HCC) is considered one of the most aggressive tumors worldwide. The consumption of lipid-enriched diets, mainly high cholesterol, induces oxidative stress and chronic inflammation, leading to HCC progression. Moreover, fatty acids and cholesterol could display differential responses on immune cells inside the tumor immune microenvironment (TIME). Tumor-associated macrophages (TAMs) represent one of the most critical leukocytes in the tumor microenvironment (TME) displaying pro-tumoral responses and one of the mainly cholesterol donors to cancer cells. Immunotherapy or cholesterol regulators, alone or combined, would represent an effective strategy for HCC treatment. Nonetheless, steatotic etiology from non-alcoholic fatty liver disease (NAFLD)-HCC tumors has been unexpectedly resulting in highly aggressive behavior.
DOI: https://doi.org/10.37349/edd.2022.00003
Aim:
Cholestasis remains a partially characterized disease. Evidence has been gained that it is a systemic disease that begins in the liver but significantly impacts other organs and systems such as the kidney, heart, and intestine, among others. One of the primary damage mechanisms is the generation of reactive oxygen species (ROS), which eventually leads to oxidative stress, impacting canalicular morphology and actin cytoskeleton changes that could worsen the problem. These characteristics are also observed in the kidney and intestine. The work focused on addressing the intestine effects of intrahepatic cholestasis induced by α-naphthyl isothiocyanate (ANIT) and the protective response of the hepatocyte growth factor (HGF).
Methods:
The 10- to 12-week-old CD1 male mice were treated with ANIT and then treated or not with HGF; intestine damage was addressed by histology, immunohistochemistry (IHC) of specific markers, oxidative stress, and apoptosis.
Results:
Results show changes in the intestine histology, particularly the colon and ileum, induced by the cholestasis. HGF treatment restored the histology presentation and reverted the oxidative damage, clearly indicating a healing response. This observation was supported by an increment in anti-inflammatory macrophages (CD163+) in the HGF treatment.
Conclusions:
The data prove that HGF induces a protective and repairing response in the intestine under cholestatic challenges.
Aim:
Cholestasis remains a partially characterized disease. Evidence has been gained that it is a systemic disease that begins in the liver but significantly impacts other organs and systems such as the kidney, heart, and intestine, among others. One of the primary damage mechanisms is the generation of reactive oxygen species (ROS), which eventually leads to oxidative stress, impacting canalicular morphology and actin cytoskeleton changes that could worsen the problem. These characteristics are also observed in the kidney and intestine. The work focused on addressing the intestine effects of intrahepatic cholestasis induced by α-naphthyl isothiocyanate (ANIT) and the protective response of the hepatocyte growth factor (HGF).
Methods:
The 10- to 12-week-old CD1 male mice were treated with ANIT and then treated or not with HGF; intestine damage was addressed by histology, immunohistochemistry (IHC) of specific markers, oxidative stress, and apoptosis.
Results:
Results show changes in the intestine histology, particularly the colon and ileum, induced by the cholestasis. HGF treatment restored the histology presentation and reverted the oxidative damage, clearly indicating a healing response. This observation was supported by an increment in anti-inflammatory macrophages (CD163+) in the HGF treatment.
Conclusions:
The data prove that HGF induces a protective and repairing response in the intestine under cholestatic challenges.
DOI: https://doi.org/10.37349/edd.2022.00004
Worldwide the number of individuals being overweight or obese has dramatically increased during the last decades, which is also associated with a similar dramatic increase of individuals afflicted with metabolic disorders like dyslipidemia, hypertension, and non-alcoholic fatty liver disease (NAFLD). Genetic predisposition may account for some of the increases in body weight and the development of metabolic disorders; however, much is probably also related to the changes in physical activity and dietary pattern. Indeed, results of epidemiological studies suggest that a ‘western-type dietary pattern’ composed of highly processed foods, sweetened foods, and beverages, all adding to a low fiber but high sugar and saturated fat intake, may increase the odd of developing overweight and metabolic disorders. Consumption of sugar, and especially, fructose has repeatedly been discussed to be a key contributor to the development of health disturbances including hypertension, dyslipidemia, insulin resistance as well as NAFLD. However, despite intense research effort, the question if and how (high) dietary fructose intake interferes with human health has not yet been fully answered also as findings are sometimes contradictory. In the present narrative review, results of recent studies assessing the effect of fructose consumption on the development of metabolic disorders including hypertension, dyslipidemia, cardiovascular diseases (CVDs), hyperinsulinemia, and NAFLD as well as underlying molecular mechanisms are reviewed, thereby, aiming to further address the question if (high) fructose intake is a trigger of metabolic diseases.
Worldwide the number of individuals being overweight or obese has dramatically increased during the last decades, which is also associated with a similar dramatic increase of individuals afflicted with metabolic disorders like dyslipidemia, hypertension, and non-alcoholic fatty liver disease (NAFLD). Genetic predisposition may account for some of the increases in body weight and the development of metabolic disorders; however, much is probably also related to the changes in physical activity and dietary pattern. Indeed, results of epidemiological studies suggest that a ‘western-type dietary pattern’ composed of highly processed foods, sweetened foods, and beverages, all adding to a low fiber but high sugar and saturated fat intake, may increase the odd of developing overweight and metabolic disorders. Consumption of sugar, and especially, fructose has repeatedly been discussed to be a key contributor to the development of health disturbances including hypertension, dyslipidemia, insulin resistance as well as NAFLD. However, despite intense research effort, the question if and how (high) dietary fructose intake interferes with human health has not yet been fully answered also as findings are sometimes contradictory. In the present narrative review, results of recent studies assessing the effect of fructose consumption on the development of metabolic disorders including hypertension, dyslipidemia, cardiovascular diseases (CVDs), hyperinsulinemia, and NAFLD as well as underlying molecular mechanisms are reviewed, thereby, aiming to further address the question if (high) fructose intake is a trigger of metabolic diseases.
DOI: https://doi.org/10.37349/edd.2022.00005
The surface of intestinal epithelial cells is covered by the brush border, which consists of densely packed cellular extrusions called microvilli. Until recently, microvilli have not been known to be interconnected. In 2014, a protein complex, called the intermicrovillar adhesion complex (IMAC) which is located at the tips of the microvilli and responsible for the regular spatial organization of the brush border, was identified. Deletion of IMAC components such as cadherin-related family member-2 (CDHR2) in mice resulted in microvillus disorganization and fanning, a structural aberration that is also found in the brush border of patients with inflammatory bowel disease. The etiology of inflammatory bowel disease has been primarily associated with dysfunctional mucosal immunity, but the discovery of the IMAC may encourage theories of an epithelial origin. Here, possible effects of the brush border on the gut barrier function and intestinal inflammation are discussed proposing that the IMAC protects against inflammation through its microvillus cross-linking function.
The surface of intestinal epithelial cells is covered by the brush border, which consists of densely packed cellular extrusions called microvilli. Until recently, microvilli have not been known to be interconnected. In 2014, a protein complex, called the intermicrovillar adhesion complex (IMAC) which is located at the tips of the microvilli and responsible for the regular spatial organization of the brush border, was identified. Deletion of IMAC components such as cadherin-related family member-2 (CDHR2) in mice resulted in microvillus disorganization and fanning, a structural aberration that is also found in the brush border of patients with inflammatory bowel disease. The etiology of inflammatory bowel disease has been primarily associated with dysfunctional mucosal immunity, but the discovery of the IMAC may encourage theories of an epithelial origin. Here, possible effects of the brush border on the gut barrier function and intestinal inflammation are discussed proposing that the IMAC protects against inflammation through its microvillus cross-linking function.
DOI: https://doi.org/10.37349/edd.2022.00006
Caspases are key factors in the regulation of the apoptotic and/or inflammatory responses, both crucial in the pathogenesis of diverse diseases. Caspase-2 is the most evolutionary conserved albeit functionally poorly defined member of the caspase family. The precise role of caspase-2 as an initiator or effector caspase is still unknown, but it has been involved in a wide variety of functions, from apoptosis to genomic stability, oxidative stress, metabolism, and cancer. However, many conflicting results render the exact function of this protease still unresolved. Although caspase-2 has several hundred substrates, the activation, processing, and activity on specific substrates remain poorly described. Recent evidence indicates that caspase-2 has a role in metabolic homeostasis and is required for lipotoxicity-induced apoptosis in hepatocytes, contributing to non-alcoholic steatohepatitis (NASH) progression towards hepatocellular carcinoma (HCC). Caspase-2 protein expression strongly localizes to injured/ballooned hepatocytes, correlating with NASH severity. Also, mice lacking caspase-2 showed protection from western diet-induced obesity, dyslipidemia, and insulin resistance. Although there are no effective therapies for NASH and HCC, the evaluation of a pan-caspase inhibitor has reached a phase I/II in clinical trials for advanced liver disease. Nevertheless, a better understanding of caspase functions with the identification of specific proteolytic substrates is essential for future therapeutic developments. Bearing in mind the pressing need to identify new targets for NASH-HCC and its metabolic-related comorbidities, and the favorable effect of caspase-2 genetic inhibition in animal models, pharmacological caspase-2 inhibition arises as a promising strategy that should be further investigated.
Caspases are key factors in the regulation of the apoptotic and/or inflammatory responses, both crucial in the pathogenesis of diverse diseases. Caspase-2 is the most evolutionary conserved albeit functionally poorly defined member of the caspase family. The precise role of caspase-2 as an initiator or effector caspase is still unknown, but it has been involved in a wide variety of functions, from apoptosis to genomic stability, oxidative stress, metabolism, and cancer. However, many conflicting results render the exact function of this protease still unresolved. Although caspase-2 has several hundred substrates, the activation, processing, and activity on specific substrates remain poorly described. Recent evidence indicates that caspase-2 has a role in metabolic homeostasis and is required for lipotoxicity-induced apoptosis in hepatocytes, contributing to non-alcoholic steatohepatitis (NASH) progression towards hepatocellular carcinoma (HCC). Caspase-2 protein expression strongly localizes to injured/ballooned hepatocytes, correlating with NASH severity. Also, mice lacking caspase-2 showed protection from western diet-induced obesity, dyslipidemia, and insulin resistance. Although there are no effective therapies for NASH and HCC, the evaluation of a pan-caspase inhibitor has reached a phase I/II in clinical trials for advanced liver disease. Nevertheless, a better understanding of caspase functions with the identification of specific proteolytic substrates is essential for future therapeutic developments. Bearing in mind the pressing need to identify new targets for NASH-HCC and its metabolic-related comorbidities, and the favorable effect of caspase-2 genetic inhibition in animal models, pharmacological caspase-2 inhibition arises as a promising strategy that should be further investigated.
DOI: https://doi.org/10.37349/edd.2022.00007
Normal hepatobiliary function depends on an adequate bile flow from the liver through the biliary tree to the gallbladder, where bile is stored and concentrated, and from the gallbladder to the duodenum when it is required for the digestive process. Interruption of this secretory function results in partial or complete cholestasis, which is accompanied by important repercussions due to the lack of bile acids in the intestine and their regurgitation from hepatocytes to blood together with potentially toxic compounds that are normally eliminated in bile. The presence of active and selective transporter proteins located at both poles of the plasma membrane of hepatocytes, cholangiocytes, and epithelial cells of the ileal mucosa, together with the ability of hepatocytes to synthesize bile acids from cholesterol, enables the so-called bile acid enterohepatic circulation, which is essential in liver and gastrointestinal tract physiology. The presence in the ducts of the biliary tree of agents reducing their luminal diameter by external compression or space-occupying obstacles, either in the duct wall or its lumen, can result in total or partial obstructive cholestasis. The clinical impact and management of cholestasis are different depending on the intrahepatic or extrahepatic location of the obstacle. Thus, surgical interventions can often be helpful in removing extrahepatic obstructions and restoring normal bile flow to the duodenum. In contrast, hepatocyte or cholangiocyte damage, either global, restricted to subcellular compartments, or more specifically affecting the elements of the canalicular secretory machinery, may result in hepatocellular cholestasis or cholangiopathies. In these cases, bile flow interruption is usually partial and, except for extremely severe cases when liver transplantation is required, these patients often treated with pharmacological agents, such as ursodeoxycholic acid (UDCA) and rifampicin. The present review gathers updated information on the etiopathogenesis and pathophysiological aspects of different types of cholestasis.
Normal hepatobiliary function depends on an adequate bile flow from the liver through the biliary tree to the gallbladder, where bile is stored and concentrated, and from the gallbladder to the duodenum when it is required for the digestive process. Interruption of this secretory function results in partial or complete cholestasis, which is accompanied by important repercussions due to the lack of bile acids in the intestine and their regurgitation from hepatocytes to blood together with potentially toxic compounds that are normally eliminated in bile. The presence of active and selective transporter proteins located at both poles of the plasma membrane of hepatocytes, cholangiocytes, and epithelial cells of the ileal mucosa, together with the ability of hepatocytes to synthesize bile acids from cholesterol, enables the so-called bile acid enterohepatic circulation, which is essential in liver and gastrointestinal tract physiology. The presence in the ducts of the biliary tree of agents reducing their luminal diameter by external compression or space-occupying obstacles, either in the duct wall or its lumen, can result in total or partial obstructive cholestasis. The clinical impact and management of cholestasis are different depending on the intrahepatic or extrahepatic location of the obstacle. Thus, surgical interventions can often be helpful in removing extrahepatic obstructions and restoring normal bile flow to the duodenum. In contrast, hepatocyte or cholangiocyte damage, either global, restricted to subcellular compartments, or more specifically affecting the elements of the canalicular secretory machinery, may result in hepatocellular cholestasis or cholangiopathies. In these cases, bile flow interruption is usually partial and, except for extremely severe cases when liver transplantation is required, these patients often treated with pharmacological agents, such as ursodeoxycholic acid (UDCA) and rifampicin. The present review gathers updated information on the etiopathogenesis and pathophysiological aspects of different types of cholestasis.
DOI: https://doi.org/10.37349/edd.2022.00008
This article belongs to the special issue CHOLESTASIS
Aim:
Probiotic bacteria consumption for improving human health and for disease prevention is still controversial. There is a need to develop functional probiotic bacteria with proven efficacy for the human gastrointestinal (GI) system. The novel bacteria will lower the steady state of constant Ethanol production may lead to gut microbiota dysbiosis and liver injuries.
Methods:
Herein engineered probiotic bacterium B. subtilis to enhance the secretion of human alcohol dehydrogenase-4 (ADH4) by fusion of signal peptides (SPs) was constructed. As a result, higher ADH4 secretion and Ethanol removal rates were observed in phoB SP transformant SP-64, compared to other transformants. The engineered ADH4 expressing probiotic B. subtilis was delivered as spores to evaluate various physiological, biochemical, and immuno-histochemical parameters of mice under a high-fat diet (HFD)-induced obesity and metabolic impairment.
Results:
The treatment ameliorated significantly weight gain, improved glucose utilization, and prevented HFD-induced pancreatic damage. Lastly, SP-64 inoculation altered the gut microbiota, and increased the Firmicutes/Bacteroides ratio, supporting better fitness under HFD.
Conclusions:
SP-64 emerged as a potential probiotic that opens a new avenue for interventions against over-nutrition-induced metabolic disorders.
Aim:
Probiotic bacteria consumption for improving human health and for disease prevention is still controversial. There is a need to develop functional probiotic bacteria with proven efficacy for the human gastrointestinal (GI) system. The novel bacteria will lower the steady state of constant Ethanol production may lead to gut microbiota dysbiosis and liver injuries.
Methods:
Herein engineered probiotic bacterium B. subtilis to enhance the secretion of human alcohol dehydrogenase-4 (ADH4) by fusion of signal peptides (SPs) was constructed. As a result, higher ADH4 secretion and Ethanol removal rates were observed in phoB SP transformant SP-64, compared to other transformants. The engineered ADH4 expressing probiotic B. subtilis was delivered as spores to evaluate various physiological, biochemical, and immuno-histochemical parameters of mice under a high-fat diet (HFD)-induced obesity and metabolic impairment.
Results:
The treatment ameliorated significantly weight gain, improved glucose utilization, and prevented HFD-induced pancreatic damage. Lastly, SP-64 inoculation altered the gut microbiota, and increased the Firmicutes/Bacteroides ratio, supporting better fitness under HFD.
Conclusions:
SP-64 emerged as a potential probiotic that opens a new avenue for interventions against over-nutrition-induced metabolic disorders.
DOI: https://doi.org/10.37349/edd.2022.00009
Several metabolic pathways are involved in the biotransformation of C27 neutral cholesterol to C24 primary bile acids (BAs), mainly cholic acid (CA) and chenodeoxycholic acid (CDCA), which are then conjugated with glycine or taurine. This process can start with the modification of the steroid ring or the shortening of the side chain and involves enzymes present in different subcellular compartments. Inborn errors affecting the biogenesis of organelles, such as peroxisomes, or the expression or function of specific enzymes of these convergent routes result in: i) the lack of mature C24-BAs, with the subsequent impairment in digestion and absorption of dietary fat and liposoluble vitamins, such as vitamin K, which may account for a deficient hepatic synthesis of several coagulation factors; ii) the accumulation of intermediate metabolites, which may affect hepatocyte physiology, causing cholestasis as a commonly shared alteration besides other deleterious hepatic events; and iii) extrahepatic clinical manifestations due to accumulation of toxic metabolites in other territories, such as the nervous system, causing neurological disorders. In general, diseases whose primary alteration is a genetic defect in BA synthesis are diagnosed in children or young individuals with a very low incidence. The symptomatology can markedly vary among individuals, ranging from mild to severe conditions. Oral therapy, based on the enrichment of the BA pool with natural C24-BAs, such as CA, CDCA, glyco-CA, or ursodeoxycholic acid (UDCA), depending on the exact deficiency causing the disease, may be beneficial in preventing life-threatening situations. In contrast, in other cases, a liver transplant is the only option for these patients. This review describes the updated information on the genetic and molecular bases of these diseases and the current approaches to achieve a selective diagnosis and specific treatment.
Several metabolic pathways are involved in the biotransformation of C27 neutral cholesterol to C24 primary bile acids (BAs), mainly cholic acid (CA) and chenodeoxycholic acid (CDCA), which are then conjugated with glycine or taurine. This process can start with the modification of the steroid ring or the shortening of the side chain and involves enzymes present in different subcellular compartments. Inborn errors affecting the biogenesis of organelles, such as peroxisomes, or the expression or function of specific enzymes of these convergent routes result in: i) the lack of mature C24-BAs, with the subsequent impairment in digestion and absorption of dietary fat and liposoluble vitamins, such as vitamin K, which may account for a deficient hepatic synthesis of several coagulation factors; ii) the accumulation of intermediate metabolites, which may affect hepatocyte physiology, causing cholestasis as a commonly shared alteration besides other deleterious hepatic events; and iii) extrahepatic clinical manifestations due to accumulation of toxic metabolites in other territories, such as the nervous system, causing neurological disorders. In general, diseases whose primary alteration is a genetic defect in BA synthesis are diagnosed in children or young individuals with a very low incidence. The symptomatology can markedly vary among individuals, ranging from mild to severe conditions. Oral therapy, based on the enrichment of the BA pool with natural C24-BAs, such as CA, CDCA, glyco-CA, or ursodeoxycholic acid (UDCA), depending on the exact deficiency causing the disease, may be beneficial in preventing life-threatening situations. In contrast, in other cases, a liver transplant is the only option for these patients. This review describes the updated information on the genetic and molecular bases of these diseases and the current approaches to achieve a selective diagnosis and specific treatment.
DOI: https://doi.org/10.37349/edd.2022.00010
This article belongs to the special issue CHOLESTASIS
During liver injury and cholestasis, the mechanisms allowing the organ to protect itself with the aim of maintaining biliary homeostasis are not completely understood. Central to their biological roles, bile acids (BAs) and their receptors constitute a signaling network with multiple molecular and cellular impacts on both liver repair and protection from BA overload. BA signal through nuclear [mainly farnesoid X receptor (FXR)] and membrane [mainly G protein-coupled BA receptor 1 (GPBAR-1), aka Takeda G protein-coupled receptor 5 (TGR5)] receptors, in which activation elicits a wide array of biological responses. So far, most of the studies have been focused on FXR signaling as hepato-protective, TGR5 being less explored to this regard. While the liver faces massive and potentially harmful BA overload during cholestasis, it is crucial to understand that BAs induce also protective responses contributing not only to reduce the inflammatory burden, but also to spare liver cells and their repair capacities. Based on the available literature, the TGR5 BA receptor protects the liver in the cholestatic context and counteracts BA overload with the aim of restoring biliary homeostasis mainly through the control of inflammatory processes, biliary epithelial barrier permeability, and BA pool composition. Mouse experimental models of cholestasis reveal that the lack of TGR5 was associated with exacerbated inflammation and necrosis, leaky biliary epithelium, and excessive BA pool hydrophobicity, resulting in biliary cell and parenchymal insult, and compromising optimal restoration of biliary homeostasis and liver repair. There are thus widely opened translational perspectives with the aim of targeting TGR5-related signaling or biological responses to trigger protection of the cholestatic liver.
During liver injury and cholestasis, the mechanisms allowing the organ to protect itself with the aim of maintaining biliary homeostasis are not completely understood. Central to their biological roles, bile acids (BAs) and their receptors constitute a signaling network with multiple molecular and cellular impacts on both liver repair and protection from BA overload. BA signal through nuclear [mainly farnesoid X receptor (FXR)] and membrane [mainly G protein-coupled BA receptor 1 (GPBAR-1), aka Takeda G protein-coupled receptor 5 (TGR5)] receptors, in which activation elicits a wide array of biological responses. So far, most of the studies have been focused on FXR signaling as hepato-protective, TGR5 being less explored to this regard. While the liver faces massive and potentially harmful BA overload during cholestasis, it is crucial to understand that BAs induce also protective responses contributing not only to reduce the inflammatory burden, but also to spare liver cells and their repair capacities. Based on the available literature, the TGR5 BA receptor protects the liver in the cholestatic context and counteracts BA overload with the aim of restoring biliary homeostasis mainly through the control of inflammatory processes, biliary epithelial barrier permeability, and BA pool composition. Mouse experimental models of cholestasis reveal that the lack of TGR5 was associated with exacerbated inflammation and necrosis, leaky biliary epithelium, and excessive BA pool hydrophobicity, resulting in biliary cell and parenchymal insult, and compromising optimal restoration of biliary homeostasis and liver repair. There are thus widely opened translational perspectives with the aim of targeting TGR5-related signaling or biological responses to trigger protection of the cholestatic liver.
DOI: https://doi.org/10.37349/edd.2022.00011
This article belongs to the special issue CHOLESTASIS
Metabolic zonation in the liver carries out the maintenance of organ and body homeostasis. Hypoxia is an inherent physiological feature of the liver and contributes to the zonal properties of the hepatic parenchyma. As a master regulator of hypoxia, the transcription factor hypoxia-inducing factor (HIF) is stabilized primarily by oxygen availability, and it is thought to contribute to steatohepatitis due to alcohol-related (ASH) and non-alcohol-related liver disease (NASH). Cholesterol has emerged as an important player in both diseases, and hypoxia increases hepatic cholesterol levels. Steroidogenic acute regulatory protein 1 (STARD1) is a mitochondrial outer membrane protein that transfers cholesterol to mitochondrial inner membrane for metabolic processing and acts as the rate-limiting step in the alternative pathway of bile acid synthesis in hepatocytes. STARD1 expression increases in ASH and NASH and determines the accumulation of cholesterol in mitochondria, which impacts the physico-chemical mitochondrial membranes properties and as a consequence impairs the activity of specific mitochondrial solute carriers, such as the 2-oxoglutarate carrier (2-OGC), limiting the exchange between cytosolic glutathione and mitochondrial 2-oxoglutarate (2-OG). Although HIF-1 is stabilized in hypoxia largely due to the requirement of prolylhydroxylases (PHDs) for oxygen to signal HIF degradation, PHDs are also dependent on 2-OG, and therefore it is conceivable that impairment of 2-OGC by STARD1-mediated cholesterol accumulation may contribute to HIF-1 stabilization due in part to decreased availability of cytosolic 2-OG. In this perspective, this review explores the interplay between HIF-1 stabilization and STARD1 induction and the potential contribution of this functional relationship to ASH and NASH.
Metabolic zonation in the liver carries out the maintenance of organ and body homeostasis. Hypoxia is an inherent physiological feature of the liver and contributes to the zonal properties of the hepatic parenchyma. As a master regulator of hypoxia, the transcription factor hypoxia-inducing factor (HIF) is stabilized primarily by oxygen availability, and it is thought to contribute to steatohepatitis due to alcohol-related (ASH) and non-alcohol-related liver disease (NASH). Cholesterol has emerged as an important player in both diseases, and hypoxia increases hepatic cholesterol levels. Steroidogenic acute regulatory protein 1 (STARD1) is a mitochondrial outer membrane protein that transfers cholesterol to mitochondrial inner membrane for metabolic processing and acts as the rate-limiting step in the alternative pathway of bile acid synthesis in hepatocytes. STARD1 expression increases in ASH and NASH and determines the accumulation of cholesterol in mitochondria, which impacts the physico-chemical mitochondrial membranes properties and as a consequence impairs the activity of specific mitochondrial solute carriers, such as the 2-oxoglutarate carrier (2-OGC), limiting the exchange between cytosolic glutathione and mitochondrial 2-oxoglutarate (2-OG). Although HIF-1 is stabilized in hypoxia largely due to the requirement of prolylhydroxylases (PHDs) for oxygen to signal HIF degradation, PHDs are also dependent on 2-OG, and therefore it is conceivable that impairment of 2-OGC by STARD1-mediated cholesterol accumulation may contribute to HIF-1 stabilization due in part to decreased availability of cytosolic 2-OG. In this perspective, this review explores the interplay between HIF-1 stabilization and STARD1 induction and the potential contribution of this functional relationship to ASH and NASH.
DOI: https://doi.org/10.37349/edd.2022.00012
