Uncommon threads: pneumopericardium complexity following liver catheter removal in pancreatic cancer
Pneumopericardium, the presence of air within the pericardial sac, is a rare but critical condition that can lead to severe complications such as tension pneumopericardium and cardiac tamponade, cau
[...] Read more.
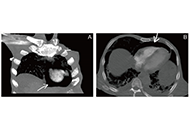
Pneumopericardium, the presence of air within the pericardial sac, is a rare but critical condition that can lead to severe complications such as tension pneumopericardium and cardiac tamponade, causing hemodynamic instability and necessitating immediate intervention. Various etiologies include congenital defects, post-surgical complications, infections, and trauma. Malignancies, such as advanced esophageal cancer or lung carcinoma, can also cause pneumopericardium via fistula formation. Multimodal imaging, including chest X-ray, echocardiography, and computed tomography (CT), is essential for diagnosis. This case report discusses a 65-year-old male with advanced pancreatic adenocarcinoma who developed pneumopericardium following the removal of a left lobe liver drainage catheter. Initial CT imaging revealed liver lesions suspicious for metastatic disease or abscess, leading to drainage procedures. Following the removal of the drainage tube, the patient experienced respiratory distress and hypotension, and computed tomography pulmonary angiogram (CTPA) revealed pneumopericardium, likely due to a fistula formed between the abscess and pericardium. Despite no echocardiographic signs of tamponade, the patient’s persistent hypotension warranted CT-guided pericardiocentesis, resulting in gradual blood pressure improvement. This case highlights the intricate interplay between malignancy, infection, and procedural complications in developing pneumopericardium. It emphasizes the need for a multidisciplinary approach and the importance of considering both the quantity and rate of air accumulation when assessing the risk of hemodynamic compromise. The patient’s hemodynamic instability and subsequent improvement following pericardiocentesis underscore the critical role of timely intervention in managing this condition.
Ahmed Basuoni ... Marwa Makhlouf
Pneumopericardium, the presence of air within the pericardial sac, is a rare but critical condition that can lead to severe complications such as tension pneumopericardium and cardiac tamponade, causing hemodynamic instability and necessitating immediate intervention. Various etiologies include congenital defects, post-surgical complications, infections, and trauma. Malignancies, such as advanced esophageal cancer or lung carcinoma, can also cause pneumopericardium via fistula formation. Multimodal imaging, including chest X-ray, echocardiography, and computed tomography (CT), is essential for diagnosis. This case report discusses a 65-year-old male with advanced pancreatic adenocarcinoma who developed pneumopericardium following the removal of a left lobe liver drainage catheter. Initial CT imaging revealed liver lesions suspicious for metastatic disease or abscess, leading to drainage procedures. Following the removal of the drainage tube, the patient experienced respiratory distress and hypotension, and computed tomography pulmonary angiogram (CTPA) revealed pneumopericardium, likely due to a fistula formed between the abscess and pericardium. Despite no echocardiographic signs of tamponade, the patient’s persistent hypotension warranted CT-guided pericardiocentesis, resulting in gradual blood pressure improvement. This case highlights the intricate interplay between malignancy, infection, and procedural complications in developing pneumopericardium. It emphasizes the need for a multidisciplinary approach and the importance of considering both the quantity and rate of air accumulation when assessing the risk of hemodynamic compromise. The patient’s hemodynamic instability and subsequent improvement following pericardiocentesis underscore the critical role of timely intervention in managing this condition.
 Uncommon threads: pneumopericardium complexity following liver catheter removal in pancreatic cancerOpen AccessCase ReportPneumopericardium, the presence of air within the pericardial sac, is a rare but critical condition that can lead to severe complications such as tension pneumopericardium and cardiac tamponade, cau [...] Read more.Ahmed Basuoni ... Marwa MakhloufPublished: August 06, 2024 Explor Cardiol. 2024;2:178–182
Uncommon threads: pneumopericardium complexity following liver catheter removal in pancreatic cancerOpen AccessCase ReportPneumopericardium, the presence of air within the pericardial sac, is a rare but critical condition that can lead to severe complications such as tension pneumopericardium and cardiac tamponade, cau [...] Read more.Ahmed Basuoni ... Marwa MakhloufPublished: August 06, 2024 Explor Cardiol. 2024;2:178–182 Vascular senescence and atherosclerotic plaque vulnerability: investigating the telomere-mitochondria crosstalk—rationale and design of the VICTORIA StudyOpen AccessProtocolVascular aging is recognized as one of the hallmarks of atherosclerosis. Currently, a growing body of evidence suggests that there exists a mutual crosstalk between telomere dysfunction and mitochon [...] Read more.Jonica Campolo ... Maria Grazia AndreassiPublished: July 24, 2024 Explor Cardiol. 2024;2:168–177
Vascular senescence and atherosclerotic plaque vulnerability: investigating the telomere-mitochondria crosstalk—rationale and design of the VICTORIA StudyOpen AccessProtocolVascular aging is recognized as one of the hallmarks of atherosclerosis. Currently, a growing body of evidence suggests that there exists a mutual crosstalk between telomere dysfunction and mitochon [...] Read more.Jonica Campolo ... Maria Grazia AndreassiPublished: July 24, 2024 Explor Cardiol. 2024;2:168–177 Percutaneous versus open cannulation for mechanical support in patients with right ventricular failure after left ventricular assist device placementOpen AccessOriginal ArticleAim: Temporary right ventricular assist device (t-RVAD) is an option for those patients in right ventricular failure (RVF) after left ventricular assist device (LVAD) resistant to ionotropic ther [...] Read more.Amit Prasad ... Behzad SoleimaniPublished: July 18, 2024 Explor Cardiol. 2024;2:158–167
Percutaneous versus open cannulation for mechanical support in patients with right ventricular failure after left ventricular assist device placementOpen AccessOriginal ArticleAim: Temporary right ventricular assist device (t-RVAD) is an option for those patients in right ventricular failure (RVF) after left ventricular assist device (LVAD) resistant to ionotropic ther [...] Read more.Amit Prasad ... Behzad SoleimaniPublished: July 18, 2024 Explor Cardiol. 2024;2:158–167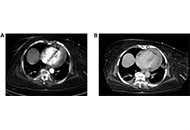 Cardiac tamponade after thrombectomyOpen AccessCase ReportPulmonary embolism (PE) is the third leading cause of cardiovascular mortality worldwide. Percutaneous mechanical thrombectomy is indicated in patients with contraindications to thrombolysis. Compli [...] Read more.Shruthi Sivakumar ... Suzette Graham-HillPublished: July 17, 2024 Explor Cardiol. 2024;2:148–157
Cardiac tamponade after thrombectomyOpen AccessCase ReportPulmonary embolism (PE) is the third leading cause of cardiovascular mortality worldwide. Percutaneous mechanical thrombectomy is indicated in patients with contraindications to thrombolysis. Compli [...] Read more.Shruthi Sivakumar ... Suzette Graham-HillPublished: July 17, 2024 Explor Cardiol. 2024;2:148–157