Valve-in-valve transcatheter aortic valve replacement: state of art
Redo surgical aortic valve replacement (SAVR) has long been the standard treatment for severe symptomatic aortic stenosis (AS) and insufficiency, but transcatheter aortic valve replacement (TAVR) ha
[...] Read more.
Redo surgical aortic valve replacement (SAVR) has long been the standard treatment for severe symptomatic aortic stenosis (AS) and insufficiency, but transcatheter aortic valve replacement (TAVR) has emerged as a less invasive alternative, particularly for symptomatic AS. With calcification being a primary mechanism behind structural valve degeneration, factors such as patient characteristics and the type of bioprosthetic valve play crucial roles in determining risk. Valve-in-valve TAVR (ViV TAVR) has gained prominence as a viable alternative to redo SAVR in recent years. Echocardiography plays a pivotal role in patient selection, procedural guidance, and post-procedural evaluation in ViV TAVR. From pre-procedural assessment using transthoracic and transesophageal echocardiography to intra-procedural guidance and post-procedural follow-up, echocardiography aids in ensuring procedural success and monitoring valve function. Decision-making between redo SAVR and ViV TAVR involves multidisciplinary teams considering various factors like patient risk profile, anatomical considerations, and technical feasibility. While redo SAVR remains preferred for younger patients with lower risk, ViV TAVR is increasingly considered for older patients or those with higher reoperation risks. Factors such as coronary artery obstruction risk, patient-prosthesis mismatch, and paravalvular leak guide treatment decisions. Procedural techniques in ViV TAVR have evolved to minimize complications and optimize outcomes. Factors like access route selection, valve choice, and procedural guidance techniques significantly impact procedural success. Balloon valve fracture and preventive strategies against coronary obstruction are crucial considerations during the procedure. Post-procedural evaluation involves assessing clinical and hemodynamic outcomes, with long-term studies indicating favorable results but highlighting the importance of careful evaluation of transprosthetic gradients and valve function. ViV TAVR offers promising outcomes but requires meticulous patient selection, procedural planning, and post-procedural management to ensure optimal results.
Marco Fabio Costantino ... Luisiana Stolfi
Redo surgical aortic valve replacement (SAVR) has long been the standard treatment for severe symptomatic aortic stenosis (AS) and insufficiency, but transcatheter aortic valve replacement (TAVR) has emerged as a less invasive alternative, particularly for symptomatic AS. With calcification being a primary mechanism behind structural valve degeneration, factors such as patient characteristics and the type of bioprosthetic valve play crucial roles in determining risk. Valve-in-valve TAVR (ViV TAVR) has gained prominence as a viable alternative to redo SAVR in recent years. Echocardiography plays a pivotal role in patient selection, procedural guidance, and post-procedural evaluation in ViV TAVR. From pre-procedural assessment using transthoracic and transesophageal echocardiography to intra-procedural guidance and post-procedural follow-up, echocardiography aids in ensuring procedural success and monitoring valve function. Decision-making between redo SAVR and ViV TAVR involves multidisciplinary teams considering various factors like patient risk profile, anatomical considerations, and technical feasibility. While redo SAVR remains preferred for younger patients with lower risk, ViV TAVR is increasingly considered for older patients or those with higher reoperation risks. Factors such as coronary artery obstruction risk, patient-prosthesis mismatch, and paravalvular leak guide treatment decisions. Procedural techniques in ViV TAVR have evolved to minimize complications and optimize outcomes. Factors like access route selection, valve choice, and procedural guidance techniques significantly impact procedural success. Balloon valve fracture and preventive strategies against coronary obstruction are crucial considerations during the procedure. Post-procedural evaluation involves assessing clinical and hemodynamic outcomes, with long-term studies indicating favorable results but highlighting the importance of careful evaluation of transprosthetic gradients and valve function. ViV TAVR offers promising outcomes but requires meticulous patient selection, procedural planning, and post-procedural management to ensure optimal results.
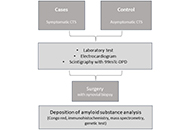 Systemic transthyretin amyloidosis: carpal tunnel syndrome in a Portuguese population (CarPoS)Open AccessProtocolCarpal tunnel syndrome (CTS) is the most common type of entrapment neuropathy and affects approximately 1% to 5% of the general population, mostly patients older than 50 years. CTS is present in var [...] Read more.Sofia Pimenta ... Elisabete MartinsPublished: October 24, 2024 Explor Cardiol. 2024;2:217–223
Systemic transthyretin amyloidosis: carpal tunnel syndrome in a Portuguese population (CarPoS)Open AccessProtocolCarpal tunnel syndrome (CTS) is the most common type of entrapment neuropathy and affects approximately 1% to 5% of the general population, mostly patients older than 50 years. CTS is present in var [...] Read more.Sofia Pimenta ... Elisabete MartinsPublished: October 24, 2024 Explor Cardiol. 2024;2:217–223 Echocardiographic findings and subsequent risk of native valve endocarditisOpen AccessOriginal ArticleAim: The association of echocardiographic findings and subsequent risk of left-sided native valve endocarditis (LS-NVE) is undefined. The aim of this study was to determine if transthoracic echoc [...] Read more.Juan A. Quintero-Martinez ... Larry M. BaddourPublished: September 24, 2024 Explor Cardiol. 2024;2:204–216
Echocardiographic findings and subsequent risk of native valve endocarditisOpen AccessOriginal ArticleAim: The association of echocardiographic findings and subsequent risk of left-sided native valve endocarditis (LS-NVE) is undefined. The aim of this study was to determine if transthoracic echoc [...] Read more.Juan A. Quintero-Martinez ... Larry M. BaddourPublished: September 24, 2024 Explor Cardiol. 2024;2:204–216 Enhancing patient care: a multimodality strategy for dilated cardiomyopathy in Chagas diseaseOpen AccessCase ReportChagas disease is a systemic illness characterized by acute and chronic phases. If untreated, it can lead to dysfunction of vital organs, notably the heart, ultimately resulting in heart failure. Tr [...] Read more.Luigy Vasquez-Yeng ... Nilda Espinola-ZavaletaPublished: September 22, 2024 Explor Cardiol. 2024;2:196–203
Enhancing patient care: a multimodality strategy for dilated cardiomyopathy in Chagas diseaseOpen AccessCase ReportChagas disease is a systemic illness characterized by acute and chronic phases. If untreated, it can lead to dysfunction of vital organs, notably the heart, ultimately resulting in heart failure. Tr [...] Read more.Luigy Vasquez-Yeng ... Nilda Espinola-ZavaletaPublished: September 22, 2024 Explor Cardiol. 2024;2:196–203 Valve-in-valve transcatheter aortic valve replacement: state of artOpen AccessReviewRedo surgical aortic valve replacement (SAVR) has long been the standard treatment for severe symptomatic aortic stenosis (AS) and insufficiency, but transcatheter aortic valve replacement (TAVR) ha [...] Read more.Marco Fabio Costantino ... Luisiana StolfiPublished: August 16, 2024 Explor Cardiol. 2024;2:183–195
Valve-in-valve transcatheter aortic valve replacement: state of artOpen AccessReviewRedo surgical aortic valve replacement (SAVR) has long been the standard treatment for severe symptomatic aortic stenosis (AS) and insufficiency, but transcatheter aortic valve replacement (TAVR) ha [...] Read more.Marco Fabio Costantino ... Luisiana StolfiPublished: August 16, 2024 Explor Cardiol. 2024;2:183–195