-
51 results in Exploration of CardiologySort byMost Cited
 Who is the author: genuine, honorary, ghost, gold, and fake authors?Open AccessEditorialWhile authorship practices can vary across different disciplines, authorship should reflect the individuals who have made a substantial contribution to the research project, take public [...] Read more.Eugenio PicanoPublished: May 13, 2024 Explor Cardiol. 2024;2:88–96
Who is the author: genuine, honorary, ghost, gold, and fake authors?Open AccessEditorialWhile authorship practices can vary across different disciplines, authorship should reflect the individuals who have made a substantial contribution to the research project, take public [...] Read more.Eugenio PicanoPublished: May 13, 2024 Explor Cardiol. 2024;2:88–96
DOI: https://doi.org/10.37349/ec.2024.00024 Noninvasive identification and therapeutic implications of supernormal left ventricular contractile phenotypeOpen AccessReviewLeft ventricular (LV) function is typically evaluated through LV ejection fraction (EF), a robust indicator of risk, showing a nonlinear increase in mortality rates below 40%. Conversely, [...] Read more.Yi Wang, Lixue YinPublished: June 17, 2024 Explor Cardiol. 2024;2:97–113
Noninvasive identification and therapeutic implications of supernormal left ventricular contractile phenotypeOpen AccessReviewLeft ventricular (LV) function is typically evaluated through LV ejection fraction (EF), a robust indicator of risk, showing a nonlinear increase in mortality rates below 40%. Conversely, [...] Read more.Yi Wang, Lixue YinPublished: June 17, 2024 Explor Cardiol. 2024;2:97–113
DOI: https://doi.org/10.37349/ec.2024.00025 Low-doses ionizing radiation exposure: an emerging causal risk factor for cardiovascular diseaseOpen AccessCommentaryMaria Grazia AndreassiPublished: December 11, 2023 Explor Cardiol. 2023;1:141–147
Low-doses ionizing radiation exposure: an emerging causal risk factor for cardiovascular diseaseOpen AccessCommentaryMaria Grazia AndreassiPublished: December 11, 2023 Explor Cardiol. 2023;1:141–147
DOI: https://doi.org/10.37349/ec.2023.00013
This article belongs to the special issue Environmental Cardiology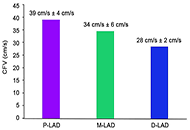 Normal physiologic coronary flow velocity gradient across the left anterior descending artery in healthy asymptomatic subjectsOpen AccessOriginal ArticleAim: Coronary flow velocity (CFV) can be obtained with transthoracic echocardiography (TTE) in the left anterior descending coronary artery (LAD). The physiologic flow velocity gradient across th [...] Read more.Fausto Rigo ... Maurizio AgnolettoPublished: August 31, 2023 Explor Cardiol. 2023;1:42–48
Normal physiologic coronary flow velocity gradient across the left anterior descending artery in healthy asymptomatic subjectsOpen AccessOriginal ArticleAim: Coronary flow velocity (CFV) can be obtained with transthoracic echocardiography (TTE) in the left anterior descending coronary artery (LAD). The physiologic flow velocity gradient across th [...] Read more.Fausto Rigo ... Maurizio AgnolettoPublished: August 31, 2023 Explor Cardiol. 2023;1:42–48
DOI: https://doi.org/10.37349/ec.2023.00006 Nanoparticles loaded with the DNA methyltransferase inhibitor SGI-1027 decrease murine atherosclerosis and inflammation in cultured human macrophagesOpen AccessOriginal ArticleAim: The DNA of the atheroma is hypermethylated relative to adjacent healthy vascular tissue. A significant portion of hypermethylated loci in the atheroma DNA map to genes related to macrophage [...] Read more.Ana Cristina Márquez-Sánchez ... Silvio ZainaPublished: April 10, 2024 Explor Cardiol. 2024;2:49–66
Nanoparticles loaded with the DNA methyltransferase inhibitor SGI-1027 decrease murine atherosclerosis and inflammation in cultured human macrophagesOpen AccessOriginal ArticleAim: The DNA of the atheroma is hypermethylated relative to adjacent healthy vascular tissue. A significant portion of hypermethylated loci in the atheroma DNA map to genes related to macrophage [...] Read more.Ana Cristina Márquez-Sánchez ... Silvio ZainaPublished: April 10, 2024 Explor Cardiol. 2024;2:49–66
DOI: https://doi.org/10.37349/ec.2024.00021 Vascular senescence and atherosclerotic plaque vulnerability: investigating the telomere-mitochondria crosstalk—rationale and design of the VICTORIA StudyOpen AccessProtocolVascular aging is recognized as one of the hallmarks of atherosclerosis. Currently, a growing body of evidence suggests that there exists a mutual crosstalk between telomere dysfunction and mitochon [...] Read more.Jonica Campolo ... Maria Grazia AndreassiPublished: July 24, 2024 Explor Cardiol. 2024;2:168–177
Vascular senescence and atherosclerotic plaque vulnerability: investigating the telomere-mitochondria crosstalk—rationale and design of the VICTORIA StudyOpen AccessProtocolVascular aging is recognized as one of the hallmarks of atherosclerosis. Currently, a growing body of evidence suggests that there exists a mutual crosstalk between telomere dysfunction and mitochon [...] Read more.Jonica Campolo ... Maria Grazia AndreassiPublished: July 24, 2024 Explor Cardiol. 2024;2:168–177
DOI: https://doi.org/10.37349/ec.2024.00030
This article belongs to the special issue Molecular Mechanisms of Cardiovascular Aging Alcohol—dose question and the weakest link in a chemical interplayOpen AccessReviewThe deleterious consequences of alcohol consumption are extensively documented across various dimensions of human health, encompassing somatic disorders such as nervous system impairments, digestive [...] Read more.Piotr Hamala, Karina Wierzbowska-DrabikPublished: August 18, 2023 Explor Cardiol. 2023;1:15–25
Alcohol—dose question and the weakest link in a chemical interplayOpen AccessReviewThe deleterious consequences of alcohol consumption are extensively documented across various dimensions of human health, encompassing somatic disorders such as nervous system impairments, digestive [...] Read more.Piotr Hamala, Karina Wierzbowska-DrabikPublished: August 18, 2023 Explor Cardiol. 2023;1:15–25
DOI: https://doi.org/10.37349/ec.2023.00003
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin Left atrium stress echocardiography: correlation between left atrial volume, function, and B-lines at rest and during stressOpen AccessOriginal ArticleAim: Left atrial volume index (LAVI), left atrial reservoir function through left atrial reservoir strain (LASr), and B-lines in lung ultrasound serve as supplementary indicators of left ventricu [...] Read more.Costantina Prota ... Quirino CiampiPublished: February 26, 2024 Explor Cardiol. 2024;2:19–30
Left atrium stress echocardiography: correlation between left atrial volume, function, and B-lines at rest and during stressOpen AccessOriginal ArticleAim: Left atrial volume index (LAVI), left atrial reservoir function through left atrial reservoir strain (LASr), and B-lines in lung ultrasound serve as supplementary indicators of left ventricu [...] Read more.Costantina Prota ... Quirino CiampiPublished: February 26, 2024 Explor Cardiol. 2024;2:19–30
DOI: https://doi.org/10.37349/ec.2024.00018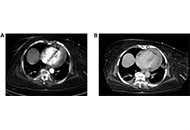 Cardiac tamponade after thrombectomyOpen AccessCase ReportPulmonary embolism (PE) is the third leading cause of cardiovascular mortality worldwide. Percutaneous mechanical thrombectomy is indicated in patients with contraindications to thrombolysis. Compli [...] Read more.Shruthi Sivakumar ... Suzette Graham-HillPublished: July 17, 2024 Explor Cardiol. 2024;2:148–157
Cardiac tamponade after thrombectomyOpen AccessCase ReportPulmonary embolism (PE) is the third leading cause of cardiovascular mortality worldwide. Percutaneous mechanical thrombectomy is indicated in patients with contraindications to thrombolysis. Compli [...] Read more.Shruthi Sivakumar ... Suzette Graham-HillPublished: July 17, 2024 Explor Cardiol. 2024;2:148–157
DOI: https://doi.org/10.37349/ec.2024.00028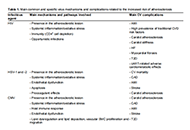 Viral infections in cardiometabolic risk and disease between old acquaintances and new enemiesOpen AccessReviewAtherosclerosis is a chronic disease, characterized by chronic inflammation, endothelial dysfunction, and lipid deposition in the vessel. Although many major, well-identified risk factors for athero [...] Read more.Cristina VassallePublished: December 27, 2023 Explor Cardiol. 2023;1:148–179
Viral infections in cardiometabolic risk and disease between old acquaintances and new enemiesOpen AccessReviewAtherosclerosis is a chronic disease, characterized by chronic inflammation, endothelial dysfunction, and lipid deposition in the vessel. Although many major, well-identified risk factors for athero [...] Read more.Cristina VassallePublished: December 27, 2023 Explor Cardiol. 2023;1:148–179
DOI: https://doi.org/10.37349/ec.2023.00014
This article belongs to the special issue Environmental Cardiology Toxic metals in pregnancy and congenital heart defects. Insights and new perspectives for a technology-driven reduction in food sourcesOpen AccessReviewCongenital heart defects (CHD) represent the most frequent congenital anomalies among newborns, as well as the leading cause of spontaneous abortion, stillbirth, neonatal and infant death. CHD have [...] Read more.Francesca Gorini, Alessandro TonacciPublished: November 13, 2023 Explor Cardiol. 2023;1:114–140
Toxic metals in pregnancy and congenital heart defects. Insights and new perspectives for a technology-driven reduction in food sourcesOpen AccessReviewCongenital heart defects (CHD) represent the most frequent congenital anomalies among newborns, as well as the leading cause of spontaneous abortion, stillbirth, neonatal and infant death. CHD have [...] Read more.Francesca Gorini, Alessandro TonacciPublished: November 13, 2023 Explor Cardiol. 2023;1:114–140
DOI: https://doi.org/10.37349/ec.2023.00012
This article belongs to the special issue Environmental Cardiology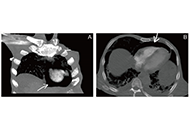 Uncommon threads: pneumopericardium complexity following liver catheter removal in pancreatic cancerOpen AccessCase ReportPneumopericardium, the presence of air within the pericardial sac, is a rare but critical condition that can lead to severe complications such as tension pneumopericardium and cardiac tamponade, cau [...] Read more.Ahmed Basuoni ... Marwa MakhloufPublished: August 06, 2024 Explor Cardiol. 2024;2:178–182
Uncommon threads: pneumopericardium complexity following liver catheter removal in pancreatic cancerOpen AccessCase ReportPneumopericardium, the presence of air within the pericardial sac, is a rare but critical condition that can lead to severe complications such as tension pneumopericardium and cardiac tamponade, cau [...] Read more.Ahmed Basuoni ... Marwa MakhloufPublished: August 06, 2024 Explor Cardiol. 2024;2:178–182
DOI: https://doi.org/10.37349/ec.2024.00031 Valve-in-valve transcatheter aortic valve replacement: state of artOpen AccessReviewRedo surgical aortic valve replacement (SAVR) has long been the standard treatment for severe symptomatic aortic stenosis (AS) and insufficiency, but transcatheter aortic valve replacement (TAVR) ha [...] Read more.Marco Fabio Costantino ... Luisiana StolfiPublished: August 16, 2024 Explor Cardiol. 2024;2:183–195
Valve-in-valve transcatheter aortic valve replacement: state of artOpen AccessReviewRedo surgical aortic valve replacement (SAVR) has long been the standard treatment for severe symptomatic aortic stenosis (AS) and insufficiency, but transcatheter aortic valve replacement (TAVR) ha [...] Read more.Marco Fabio Costantino ... Luisiana StolfiPublished: August 16, 2024 Explor Cardiol. 2024;2:183–195
DOI: https://doi.org/10.37349/ec.2024.00032 Enhancing patient care: a multimodality strategy for dilated cardiomyopathy in Chagas diseaseOpen AccessCase ReportChagas disease is a systemic illness characterized by acute and chronic phases. If untreated, it can lead to dysfunction of vital organs, notably the heart, ultimately resulting in heart failure. Tr [...] Read more.Luigy Vasquez-Yeng ... Nilda Espinola-ZavaletaPublished: September 22, 2024 Explor Cardiol. 2024;2:196–203
Enhancing patient care: a multimodality strategy for dilated cardiomyopathy in Chagas diseaseOpen AccessCase ReportChagas disease is a systemic illness characterized by acute and chronic phases. If untreated, it can lead to dysfunction of vital organs, notably the heart, ultimately resulting in heart failure. Tr [...] Read more.Luigy Vasquez-Yeng ... Nilda Espinola-ZavaletaPublished: September 22, 2024 Explor Cardiol. 2024;2:196–203
DOI: https://doi.org/10.37349/ec.2024.00033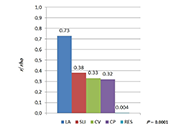 In search of heart barometer—advantage of left atrial dimension over electrocardiographic indices of left ventricular hypertrophy in arterial hypertensionOpen AccessOriginal ArticleAim: Left ventricular (LV) hypertrophy (LVH) is a common and relevant complication of arterial hypertension (AH) and 12-lead electrocardiogram (ECG) is widely used for its preliminary assessment. [...] Read more.Bogusława Nowak ... Karina Wierzbowska-DrabikPublished: July 14, 2023 Explor Cardiol. 2023;1:4–14
In search of heart barometer—advantage of left atrial dimension over electrocardiographic indices of left ventricular hypertrophy in arterial hypertensionOpen AccessOriginal ArticleAim: Left ventricular (LV) hypertrophy (LVH) is a common and relevant complication of arterial hypertension (AH) and 12-lead electrocardiogram (ECG) is widely used for its preliminary assessment. [...] Read more.Bogusława Nowak ... Karina Wierzbowska-DrabikPublished: July 14, 2023 Explor Cardiol. 2023;1:4–14
DOI: https://doi.org/10.37349/ec.2023.00002
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin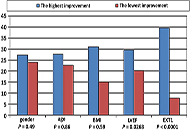 Left ventricular systolic function and initial exercise capacity—their importance for results of cardiac rehabilitation after acute coronary syndromeOpen AccessOriginal ArticleAim: The aim of this study was to compare initial and final exercise tolerance and to evaluate the determinants of exercise capacity improvement—after three weeks of inpatient cardiac rehabilit [...] Read more.Barbara Uznańska-Loch ... Tomasz RechcińskiPublished: August 30, 2023 Explor Cardiol. 2023;1:26–34
Left ventricular systolic function and initial exercise capacity—their importance for results of cardiac rehabilitation after acute coronary syndromeOpen AccessOriginal ArticleAim: The aim of this study was to compare initial and final exercise tolerance and to evaluate the determinants of exercise capacity improvement—after three weeks of inpatient cardiac rehabilit [...] Read more.Barbara Uznańska-Loch ... Tomasz RechcińskiPublished: August 30, 2023 Explor Cardiol. 2023;1:26–34
DOI: https://doi.org/10.37349/ec.2023.00004
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin Alcohol zero: the end, the beginning of the end, or just the end of the beginning?Open AccessPerspectiveAlcohol drinks, especially wine, have been described since 6,000 B.C. For many years in modern medicine, wine in moderation has been considered healthy for cardiovascular prevention, i.e., recommend [...] Read more.Miodrag Ostojic ... Dusko VulicPublished: August 31, 2023 Explor Cardiol. 2023;1:35–41
Alcohol zero: the end, the beginning of the end, or just the end of the beginning?Open AccessPerspectiveAlcohol drinks, especially wine, have been described since 6,000 B.C. For many years in modern medicine, wine in moderation has been considered healthy for cardiovascular prevention, i.e., recommend [...] Read more.Miodrag Ostojic ... Dusko VulicPublished: August 31, 2023 Explor Cardiol. 2023;1:35–41
DOI: https://doi.org/10.37349/ec.2023.00005 Exploration of Cardiology: a new journal is bornOpen AccessEditorialEugenio PicanoPublished: July 01, 2023 Explor Cardiol. 2023;1:1–3
Exploration of Cardiology: a new journal is bornOpen AccessEditorialEugenio PicanoPublished: July 01, 2023 Explor Cardiol. 2023;1:1–3
DOI: https://doi.org/10.37349/ec.2023.00001 Coronary myocardial bridge imaging by stress-echocardiography and coronary adipose tissue attenuation on computed tomography angiographyOpen AccessPerspectiveMyocardial bridging is a congenital defect characterized by the course of a segment of the coronary arteries within the heart muscle most frequently affecting the left anterior descending coronary a [...] Read more.Domenico Tuttolomondo ... Nicola GaibazziPublished: February 29, 2024 Explor Cardiol. 2024;2:31–39
Coronary myocardial bridge imaging by stress-echocardiography and coronary adipose tissue attenuation on computed tomography angiographyOpen AccessPerspectiveMyocardial bridging is a congenital defect characterized by the course of a segment of the coronary arteries within the heart muscle most frequently affecting the left anterior descending coronary a [...] Read more.Domenico Tuttolomondo ... Nicola GaibazziPublished: February 29, 2024 Explor Cardiol. 2024;2:31–39
DOI: https://doi.org/10.37349/ec.2024.00019 Role of cardio-ankle vascular index as a predictor of left ventricular hypertrophy in the evaluation of pediatric hypertensionOpen AccessOriginal ArticleAim: Cardio-ankle vascular index (CAVI) is a marker of arterial stiffness independent of blood pressure (BP) at the time of measurement. This work sought to evaluate the association of CAVI with [...] Read more.Evan Harvey ... Ranjit PhilipPublished: April 06, 2024 Explor Cardiol. 2024;2:40–48
Role of cardio-ankle vascular index as a predictor of left ventricular hypertrophy in the evaluation of pediatric hypertensionOpen AccessOriginal ArticleAim: Cardio-ankle vascular index (CAVI) is a marker of arterial stiffness independent of blood pressure (BP) at the time of measurement. This work sought to evaluate the association of CAVI with [...] Read more.Evan Harvey ... Ranjit PhilipPublished: April 06, 2024 Explor Cardiol. 2024;2:40–48
DOI: https://doi.org/10.37349/ec.2024.00020
This article belongs to the special issue Environmental Cardiology -
