The diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) in children
Over the last two decades, immunoglobulin G (IgG) antibodies against myelin oligodendrocyte glycoprotein (MOG), previously thought to be a biomarker of multiple sclerosis (MS), have been shown to ca
[...] Read more.
Over the last two decades, immunoglobulin G (IgG) antibodies against myelin oligodendrocyte glycoprotein (MOG), previously thought to be a biomarker of multiple sclerosis (MS), have been shown to cause a distinct disease called MOG antibody-associated disease (MOGAD). MOGAD accounts for approximately one-third of all demyelinating syndromes in children and is the second most common central nervous system (CNS) demyelinating disease after MS. The diagnosis is made by detecting anti-MOG IgG antibodies against the natural MOG antigen, in the presence of compatible clinical and neuroradiological features. However, due to controversies in the methodologies for detecting anti-MOG antibodies and their diagnostic cutoff values, as well as the expanding clinical spectrum, accurate diagnosis may be challenging, at least in a subset of patients. Clinical presentations of MOGAD vary by age; the highest rates are seen in acute disseminated encephalomyelitis in younger children and optic neuritis, myelitis, or brainstem symptoms in older children. Although it was previously thought to be a milder demyelinating disorder and to have a monophasic course in the majority of patients, recent studies have shown that relapses occur in about half of the patients and sequelae develop in a significant proportion of them, especially in those with persistently high antibody titers, leukodystrophy-like magnetic resonance imaging (MRI) lesions, and spinal cord involvement. However, due to the monophasic course in about half of the patients, long-term treatment is not recommended after the first clinical episode but is recommended for patients who experience relapse. Accurate and early diagnosis of MOGAD is essential for proper management and better outcome. This review covers the challenges in the diagnosis of MOGAD in children.
Ünsal Yılmaz
View:1859
Download:71
Times Cited: 0
Over the last two decades, immunoglobulin G (IgG) antibodies against myelin oligodendrocyte glycoprotein (MOG), previously thought to be a biomarker of multiple sclerosis (MS), have been shown to cause a distinct disease called MOG antibody-associated disease (MOGAD). MOGAD accounts for approximately one-third of all demyelinating syndromes in children and is the second most common central nervous system (CNS) demyelinating disease after MS. The diagnosis is made by detecting anti-MOG IgG antibodies against the natural MOG antigen, in the presence of compatible clinical and neuroradiological features. However, due to controversies in the methodologies for detecting anti-MOG antibodies and their diagnostic cutoff values, as well as the expanding clinical spectrum, accurate diagnosis may be challenging, at least in a subset of patients. Clinical presentations of MOGAD vary by age; the highest rates are seen in acute disseminated encephalomyelitis in younger children and optic neuritis, myelitis, or brainstem symptoms in older children. Although it was previously thought to be a milder demyelinating disorder and to have a monophasic course in the majority of patients, recent studies have shown that relapses occur in about half of the patients and sequelae develop in a significant proportion of them, especially in those with persistently high antibody titers, leukodystrophy-like magnetic resonance imaging (MRI) lesions, and spinal cord involvement. However, due to the monophasic course in about half of the patients, long-term treatment is not recommended after the first clinical episode but is recommended for patients who experience relapse. Accurate and early diagnosis of MOGAD is essential for proper management and better outcome. This review covers the challenges in the diagnosis of MOGAD in children.
 Analysis of congenital Zika syndrome clinicopathologic findings reported in the 8 years since the Brazilian outbreakOpen AccessSystematic ReviewAim: A Zika virus outbreak that began in Brazil, developed into an international public health emergency that extended from February 2015 until November 2016. Zika-infected pregnant women gave bi [...] Read more.Dhaara Shah ... Rana ZeinePublished: February 27, 2024 Explor Neuroprot Ther. 2024;4:82–99
Analysis of congenital Zika syndrome clinicopathologic findings reported in the 8 years since the Brazilian outbreakOpen AccessSystematic ReviewAim: A Zika virus outbreak that began in Brazil, developed into an international public health emergency that extended from February 2015 until November 2016. Zika-infected pregnant women gave bi [...] Read more.Dhaara Shah ... Rana ZeinePublished: February 27, 2024 Explor Neuroprot Ther. 2024;4:82–99 Carbon nanotubes as neuroprotective agentsOpen AccessReviewCarbon nanotubes, an emerging class of carbon nanomaterials, possess tremendous potential for application in biotechnology and biomedicine particularly in neurological disorders. Carbon nanotubes ow [...] Read more.Daisy L. Wilson ... Mahesh NarayanPublished: February 27, 2024 Explor Neuroprot Ther. 2024;4:72–81
Carbon nanotubes as neuroprotective agentsOpen AccessReviewCarbon nanotubes, an emerging class of carbon nanomaterials, possess tremendous potential for application in biotechnology and biomedicine particularly in neurological disorders. Carbon nanotubes ow [...] Read more.Daisy L. Wilson ... Mahesh NarayanPublished: February 27, 2024 Explor Neuroprot Ther. 2024;4:72–81 Advances in neuroprotective therapy for acute ischemic strokeOpen AccessReviewAcute ischemic stroke (AIS) is the leading cause of disability worldwide, and recanalization therapy is primary in the hyperacute phase of AIS. However, reperfusion injury and hemorrhagic transforma [...] Read more.Yang Yang ... Yi LiPublished: February 27, 2024 Explor Neuroprot Ther. 2024;4:55–71
Advances in neuroprotective therapy for acute ischemic strokeOpen AccessReviewAcute ischemic stroke (AIS) is the leading cause of disability worldwide, and recanalization therapy is primary in the hyperacute phase of AIS. However, reperfusion injury and hemorrhagic transforma [...] Read more.Yang Yang ... Yi LiPublished: February 27, 2024 Explor Neuroprot Ther. 2024;4:55–71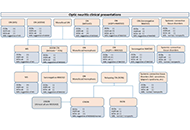 The diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) in childrenOpen AccessReviewOver the last two decades, immunoglobulin G (IgG) antibodies against myelin oligodendrocyte glycoprotein (MOG), previously thought to be a biomarker of multiple sclerosis (MS), have been shown to ca [...] Read more.Ünsal YılmazPublished: February 27, 2024 Explor Neuroprot Ther. 2024;4:38–54
The diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) in childrenOpen AccessReviewOver the last two decades, immunoglobulin G (IgG) antibodies against myelin oligodendrocyte glycoprotein (MOG), previously thought to be a biomarker of multiple sclerosis (MS), have been shown to ca [...] Read more.Ünsal YılmazPublished: February 27, 2024 Explor Neuroprot Ther. 2024;4:38–54 Resolving a paradox: antidepressants, neuroinflammation, and neurodegenerationOpen AccessReviewDepression is a known risk factor for dementia. Antidepressants are the most commonly used treatment for this condition, and are effective in at least half to two-thirds of cases. Extensive evidence [...] Read more.Ravi Philip RajkumarPublished: February 23, 2024 Explor Neuroprot Ther. 2024;4:11–37
Resolving a paradox: antidepressants, neuroinflammation, and neurodegenerationOpen AccessReviewDepression is a known risk factor for dementia. Antidepressants are the most commonly used treatment for this condition, and are effective in at least half to two-thirds of cases. Extensive evidence [...] Read more.Ravi Philip RajkumarPublished: February 23, 2024 Explor Neuroprot Ther. 2024;4:11–37 Therapeutic exercise in fibromyalgia syndrome: a narrative reviewOpen AccessReviewFibromyalgia syndrome (FMS) is characterised by the presence of distributed pain in different areas of the body accompanied by the alteration of some functions such as the activity of the neuroveget [...] Read more.Carlos Forner-Álvarez ... Núria Sempere-RubioPublished: February 20, 2024 Explor Neuroprot Ther. 2024;4:1–10
Therapeutic exercise in fibromyalgia syndrome: a narrative reviewOpen AccessReviewFibromyalgia syndrome (FMS) is characterised by the presence of distributed pain in different areas of the body accompanied by the alteration of some functions such as the activity of the neuroveget [...] Read more.Carlos Forner-Álvarez ... Núria Sempere-RubioPublished: February 20, 2024 Explor Neuroprot Ther. 2024;4:1–10