Uric acid in atherosclerosis and cardiovascular diseases: innocent bystander or ruthless killer?
Medical attention to uric acid (UA) has been increasing in recent years, mainly because this molecule has been shown to be associated with increased cardiovascular risk, both in the general populati
[...] Read more.
Medical attention to uric acid (UA) has been increasing in recent years, mainly because this molecule has been shown to be associated with increased cardiovascular risk, both in the general population and in the hypertensive patients. A growing body of clinical and experimental data supports this view and prompts reconsideration of the role of UA in the development of atherosclerosis and the genesis of cardiovascular disease. It is known that this substance, in certain plasma concentrations, induces increased oxidative stress, a chronic inflammatory state, and a whole series of other modifications that are potentially deleterious at the cardiovascular level leading to hypertension, atherosclerosis, atrial fibrillation (AF), and other metabolic changes such as diabetes, metabolic syndrome, non-alcoholic fatty liver disease and kidney failure. Despite this epidemiologic and mechanistic evidence, the current guidelines from international cardiology scientific societies do not give precise indications in this regard, and some of them only suggest UA evaluation as part of an initial screening of the hypertensive patient. The purpose of this review is to briefly describe the main clinical and epidemiological evidence supporting the role of hyperuricemia as a possible emerging cardiovascular risk factor and to analyze the potential pathophysiological mechanisms through which elevated UA levels may exert a detrimental effect on the cardiovascular system.
Giovanni Cimmino ... Plinio Cirillo
View:1202
Download:57
Times Cited: 0
Medical attention to uric acid (UA) has been increasing in recent years, mainly because this molecule has been shown to be associated with increased cardiovascular risk, both in the general population and in the hypertensive patients. A growing body of clinical and experimental data supports this view and prompts reconsideration of the role of UA in the development of atherosclerosis and the genesis of cardiovascular disease. It is known that this substance, in certain plasma concentrations, induces increased oxidative stress, a chronic inflammatory state, and a whole series of other modifications that are potentially deleterious at the cardiovascular level leading to hypertension, atherosclerosis, atrial fibrillation (AF), and other metabolic changes such as diabetes, metabolic syndrome, non-alcoholic fatty liver disease and kidney failure. Despite this epidemiologic and mechanistic evidence, the current guidelines from international cardiology scientific societies do not give precise indications in this regard, and some of them only suggest UA evaluation as part of an initial screening of the hypertensive patient. The purpose of this review is to briefly describe the main clinical and epidemiological evidence supporting the role of hyperuricemia as a possible emerging cardiovascular risk factor and to analyze the potential pathophysiological mechanisms through which elevated UA levels may exert a detrimental effect on the cardiovascular system.
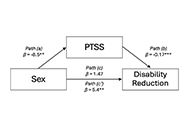 Sex differences in response to rehabilitation treatment for musculoskeletal pain: the mediating role of post-traumatic stress symptomsOpen AccessOriginal ArticleAim: Numerous investigations have revealed sex differences in recovery outcomes in individuals who have sustained work-related musculoskeletal injuries (WRMIs). Previous research has also reveale [...] Read more.Antonina D.S. Pavilanis ... Michael J.L. SullivanPublished: June 26, 2024 Explor Musculoskeletal Dis. 2024;2:242–255
Sex differences in response to rehabilitation treatment for musculoskeletal pain: the mediating role of post-traumatic stress symptomsOpen AccessOriginal ArticleAim: Numerous investigations have revealed sex differences in recovery outcomes in individuals who have sustained work-related musculoskeletal injuries (WRMIs). Previous research has also reveale [...] Read more.Antonina D.S. Pavilanis ... Michael J.L. SullivanPublished: June 26, 2024 Explor Musculoskeletal Dis. 2024;2:242–255 How to treat a patient with psoriatic arthritis and chronic lymphocytic leukemia?Open AccessCase ReportA 76-year-old male patient who has been suffering from psoriatic arthritis (PsA) for 15 years was diagnosed with chronic lymphocytic leukemia (CLL) 18 months ago. He has been treated him with a Brut [...] Read more.Jürgen Braun ... Denis PoddubnyyPublished: June 20, 2024 Explor Musculoskeletal Dis. 2024;2:235–241
How to treat a patient with psoriatic arthritis and chronic lymphocytic leukemia?Open AccessCase ReportA 76-year-old male patient who has been suffering from psoriatic arthritis (PsA) for 15 years was diagnosed with chronic lymphocytic leukemia (CLL) 18 months ago. He has been treated him with a Brut [...] Read more.Jürgen Braun ... Denis PoddubnyyPublished: June 20, 2024 Explor Musculoskeletal Dis. 2024;2:235–241 Obesity in rheumatoid arthritis: impact on response to biologic therapiesOpen AccessSystematic ReviewBackground: We performed a service evaluation of local patients with rheumatoid arthritis (RA) treated with biologic or targeted systemic disease-modifying anti-rheumatic drug (b/ts)DMARDs to see [...] Read more.Zehra Irshad, Nicola J. GullickPublished: June 12, 2024 Explor Musculoskeletal Dis. 2024;2:216–234
Obesity in rheumatoid arthritis: impact on response to biologic therapiesOpen AccessSystematic ReviewBackground: We performed a service evaluation of local patients with rheumatoid arthritis (RA) treated with biologic or targeted systemic disease-modifying anti-rheumatic drug (b/ts)DMARDs to see [...] Read more.Zehra Irshad, Nicola J. GullickPublished: June 12, 2024 Explor Musculoskeletal Dis. 2024;2:216–234 Universal screening for developmental dysplasia of the hip in Austria: what have we learned?Open AccessPerspectiveHip ultrasound, according to Graf, is a standardized sonographic method for the detection of developmental dysplasia of the hip (DDH) during the neonatal period. Graf established his method during t [...] Read more.Tanja Kraus, Catharina ChiariPublished: June 03, 2024 Explor Musculoskeletal Dis. 2024;2:208–215
Universal screening for developmental dysplasia of the hip in Austria: what have we learned?Open AccessPerspectiveHip ultrasound, according to Graf, is a standardized sonographic method for the detection of developmental dysplasia of the hip (DDH) during the neonatal period. Graf established his method during t [...] Read more.Tanja Kraus, Catharina ChiariPublished: June 03, 2024 Explor Musculoskeletal Dis. 2024;2:208–215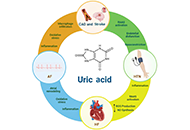 Uric acid in atherosclerosis and cardiovascular diseases: innocent bystander or ruthless killer?Open AccessReviewMedical attention to uric acid (UA) has been increasing in recent years, mainly because this molecule has been shown to be associated with increased cardiovascular risk, both in the general populati [...] Read more.Giovanni Cimmino ... Plinio CirilloPublished: June 03, 2024 Explor Musculoskeletal Dis. 2024;2:189–207
Uric acid in atherosclerosis and cardiovascular diseases: innocent bystander or ruthless killer?Open AccessReviewMedical attention to uric acid (UA) has been increasing in recent years, mainly because this molecule has been shown to be associated with increased cardiovascular risk, both in the general populati [...] Read more.Giovanni Cimmino ... Plinio CirilloPublished: June 03, 2024 Explor Musculoskeletal Dis. 2024;2:189–207 A systematic review of DDH screening practices in the UKOpen AccessSystematic ReviewBackground: The United Kingdom (UK) currently employs a selective screening system for developmental dysplasia of the hip (DDH). Despite this, late presentation rates remain high. The aim of this [...] Read more.Nicholas Birkett ... Claudia MaizenPublished: June 03, 2024 Explor Musculoskeletal Dis. 2024;2:181–188
A systematic review of DDH screening practices in the UKOpen AccessSystematic ReviewBackground: The United Kingdom (UK) currently employs a selective screening system for developmental dysplasia of the hip (DDH). Despite this, late presentation rates remain high. The aim of this [...] Read more.Nicholas Birkett ... Claudia MaizenPublished: June 03, 2024 Explor Musculoskeletal Dis. 2024;2:181–188 Mesenchymal stromal cells from people with osteoporosis are fewer, and defective in both osteogenic and adipogenic capacityOpen AccessOriginal ArticleAim: Osteoporosis (OP) is caused by imbalanced bone remodelling homeostasis. It is highly prevalent, especially in post-menopausal women, resulting in high risk of fracture and morbidity. Mesench [...] Read more.Féaron C. Cassidy ... Cynthia M. ColemanPublished: June 03, 2024 Explor Musculoskeletal Dis. 2024;2:164–180
Mesenchymal stromal cells from people with osteoporosis are fewer, and defective in both osteogenic and adipogenic capacityOpen AccessOriginal ArticleAim: Osteoporosis (OP) is caused by imbalanced bone remodelling homeostasis. It is highly prevalent, especially in post-menopausal women, resulting in high risk of fracture and morbidity. Mesench [...] Read more.Féaron C. Cassidy ... Cynthia M. ColemanPublished: June 03, 2024 Explor Musculoskeletal Dis. 2024;2:164–180 The reality of sonography of the infant hip in Brazil: results and recommendationsOpen AccessReviewSince 1980, when Professor Reinhard Graf developed a novel technique, sonography of the infant hip has played a prominent role in the early diagnosis of developmental dysplasia of the hip (DDH). Bra [...] Read more.Giovanna Galvão Braga Motta ... Alexandre Francisco de LourençoPublished: May 20, 2024 Explor Musculoskeletal Dis. 2024;2:156–163
The reality of sonography of the infant hip in Brazil: results and recommendationsOpen AccessReviewSince 1980, when Professor Reinhard Graf developed a novel technique, sonography of the infant hip has played a prominent role in the early diagnosis of developmental dysplasia of the hip (DDH). Bra [...] Read more.Giovanna Galvão Braga Motta ... Alexandre Francisco de LourençoPublished: May 20, 2024 Explor Musculoskeletal Dis. 2024;2:156–163 Validation of computer-based analysis of static ultrasound images of patellar and Achilles tendon enthesis territoriesOpen AccessOriginal ArticleAim: The aim of the present study is to conduct interobserver and intra-observer validation of computer analysis of static ultrasound images of entheseal territories of the Achilles and distal pa [...] Read more.Carlos A. Guillén-Astete ... Mónica Vázquez-DíazPublished: May 15, 2024 Explor Musculoskeletal Dis. 2024;2:148–155
Validation of computer-based analysis of static ultrasound images of patellar and Achilles tendon enthesis territoriesOpen AccessOriginal ArticleAim: The aim of the present study is to conduct interobserver and intra-observer validation of computer analysis of static ultrasound images of entheseal territories of the Achilles and distal pa [...] Read more.Carlos A. Guillén-Astete ... Mónica Vázquez-DíazPublished: May 15, 2024 Explor Musculoskeletal Dis. 2024;2:148–155 Hip sonography in SwitzerlandOpen AccessPerspectiveThe diagnosis of hip dysplasia has developed very differently in different countries over the last few decades. The development and current situation in Switzerland is described in this paper. In th [...] Read more.Beat DubsPublished: May 15, 2024 Explor Musculoskeletal Dis. 2024;2:145–147
Hip sonography in SwitzerlandOpen AccessPerspectiveThe diagnosis of hip dysplasia has developed very differently in different countries over the last few decades. The development and current situation in Switzerland is described in this paper. In th [...] Read more.Beat DubsPublished: May 15, 2024 Explor Musculoskeletal Dis. 2024;2:145–147