-
8 results in Exploration of MedicineSort byLatest
 High salt induced augmentation of angiotensin II mediated hypertension is associated with differential expression of tumor necrosis factor-alpha receptors in the kidneyOpen AccessOriginal ArticleAim: Chronic high salt (HS) intake causes minimal changes in blood pressure (BP) but it induces augmented hypertensive response to angiotensin II (AngII) administration in rodents. The mechanism [...] Read more.Dewan S. A. Majid ... L. Gabriel NavarPublished: April 26, 2022 Explor Med. 2022;3:205–218
High salt induced augmentation of angiotensin II mediated hypertension is associated with differential expression of tumor necrosis factor-alpha receptors in the kidneyOpen AccessOriginal ArticleAim: Chronic high salt (HS) intake causes minimal changes in blood pressure (BP) but it induces augmented hypertensive response to angiotensin II (AngII) administration in rodents. The mechanism [...] Read more.Dewan S. A. Majid ... L. Gabriel NavarPublished: April 26, 2022 Explor Med. 2022;3:205–218
DOI: https://doi.org/10.37349/emed.2022.00086
This article belongs to the special issue Angiotensins—A Century of Progress Reactive oxygen species in cardiovascular diseases: an updateOpen AccessReviewCardiovascular diseases are among the leading causes of death worldwide, imposing major health threats. Reactive oxygen species (ROS) are one of the most important products from the process of redox [...] Read more.Juanjuan Fei ... Jun RenPublished: April 26, 2022 Explor Med. 2022;3:188–204
Reactive oxygen species in cardiovascular diseases: an updateOpen AccessReviewCardiovascular diseases are among the leading causes of death worldwide, imposing major health threats. Reactive oxygen species (ROS) are one of the most important products from the process of redox [...] Read more.Juanjuan Fei ... Jun RenPublished: April 26, 2022 Explor Med. 2022;3:188–204
DOI: https://doi.org/10.37349/emed.2022.00085
This article belongs to the special issue Reactive Oxygen Species (ROS) in Pathophysiological Conditions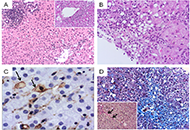 Complex liver injury induced by combined Aloe Vera and vitamin A oral supplements, as assessed by histology and the updated RUCAMOpen AccessCase ReportA case of combined acute and chronic liver injury related to consumption of multi-ingredient nutritional oral supplements containing Aloe Vera gel and vitamin A among other vitamins, minerals and di [...] Read more.Katerina Delladetsima ... Stratigoula SakellariouPublished: April 24, 2022 Explor Med. 2022;3:181–187
Complex liver injury induced by combined Aloe Vera and vitamin A oral supplements, as assessed by histology and the updated RUCAMOpen AccessCase ReportA case of combined acute and chronic liver injury related to consumption of multi-ingredient nutritional oral supplements containing Aloe Vera gel and vitamin A among other vitamins, minerals and di [...] Read more.Katerina Delladetsima ... Stratigoula SakellariouPublished: April 24, 2022 Explor Med. 2022;3:181–187
DOI: https://doi.org/10.37349/emed.2022.00084
This article belongs to the special issue Exploring Chronic Liver Disease Semaglutide: a game changer for metabolic diseases?Open AccessCommentarySemaglutide is a glucagon-like peptide 1 receptor agonist (GLP-1 RA) molecule approved for the treatment of both type 2 diabetes (T2D) and obesity. Semaglutide has a greater impact on glycated haemo [...] Read more.Agostino Milluzzo ... Laura SciaccaPublished: April 19, 2022 Explor Med. 2022;3:173–180
Semaglutide: a game changer for metabolic diseases?Open AccessCommentarySemaglutide is a glucagon-like peptide 1 receptor agonist (GLP-1 RA) molecule approved for the treatment of both type 2 diabetes (T2D) and obesity. Semaglutide has a greater impact on glycated haemo [...] Read more.Agostino Milluzzo ... Laura SciaccaPublished: April 19, 2022 Explor Med. 2022;3:173–180
DOI: https://doi.org/10.37349/emed.2022.00083 Development of systolic dysfunction unrelated to myocardial infarction in treated hypertensive patients with left ventricular hypertrophy. The LIFE StudyOpen AccessOriginal ArticleAim: While it is commonly thought that left ventricular (LV) systolic function may insidiously deteriorate in hypertensive patients, few prospective data are available to support this notion. [...] Read more.Marcello Chinali ... Richard B. DevereuxPublished: April 02, 2022 Explor Med. 2022;3:160–172
Development of systolic dysfunction unrelated to myocardial infarction in treated hypertensive patients with left ventricular hypertrophy. The LIFE StudyOpen AccessOriginal ArticleAim: While it is commonly thought that left ventricular (LV) systolic function may insidiously deteriorate in hypertensive patients, few prospective data are available to support this notion. [...] Read more.Marcello Chinali ... Richard B. DevereuxPublished: April 02, 2022 Explor Med. 2022;3:160–172
DOI: https://doi.org/10.37349/emed.2022.00082
This article belongs to the special issue Angiotensins—A Century of Progress Incident left bundle branch block predicts cardiovascular events and death in hypertensive patients with left ventricular hypertrophy. The LIFE StudyOpen AccessOriginal ArticleAim: Whether incident left bundle branch block (LBBB) is associated with increased cardiovascular (CV) morbidity and mortality in treated hypertensive patients with left ventricular hypertrophy ( [...] Read more.Casper N. Bang ... Peter M. OkinPublished: March 29, 2022 Explor Med. 2022;3:149–159
Incident left bundle branch block predicts cardiovascular events and death in hypertensive patients with left ventricular hypertrophy. The LIFE StudyOpen AccessOriginal ArticleAim: Whether incident left bundle branch block (LBBB) is associated with increased cardiovascular (CV) morbidity and mortality in treated hypertensive patients with left ventricular hypertrophy ( [...] Read more.Casper N. Bang ... Peter M. OkinPublished: March 29, 2022 Explor Med. 2022;3:149–159
DOI: https://doi.org/10.37349/emed.2022.00081
This article belongs to the special issue Angiotensins—A Century of Progress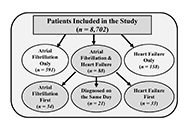 Incident atrial fibrillation and heart failure in treated hypertensive patients with left ventricular hypertrophy. The LIFE StudyOpen AccessOriginal ArticleAim: The present study investigated the appearance and severity of atrial fibrillation (AF) and heart failure (HF) in 8,702 hypertensive patients with left ventricular hypertrophy (LVH) receiving [...] Read more.Casper N. Bang ... Peter M. OkinPublished: March 23, 2022 Explor Med. 2022;3:139–148
Incident atrial fibrillation and heart failure in treated hypertensive patients with left ventricular hypertrophy. The LIFE StudyOpen AccessOriginal ArticleAim: The present study investigated the appearance and severity of atrial fibrillation (AF) and heart failure (HF) in 8,702 hypertensive patients with left ventricular hypertrophy (LVH) receiving [...] Read more.Casper N. Bang ... Peter M. OkinPublished: March 23, 2022 Explor Med. 2022;3:139–148
DOI: https://doi.org/10.37349/emed.2022.00080
This article belongs to the special issue Angiotensins—A Century of Progress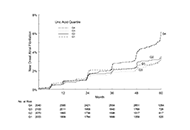 Time-varying serum uric acid predicts new-onset atrial fibrillation in treated hypertensive patients. The LIFE StudyOpen AccessOriginal ArticleAim: The Losartan Intervention For Endpoint reduction in hypertension (LIFE) study showed less new-onset atrial fibrillation (AF) in hypertensive patients receiving losartan- vs. atenolol-based t [...] Read more.Eran S. Zacks ... Richard B. DevereuxPublished: March 17, 2022 Explor Med. 2022;3:128–138
Time-varying serum uric acid predicts new-onset atrial fibrillation in treated hypertensive patients. The LIFE StudyOpen AccessOriginal ArticleAim: The Losartan Intervention For Endpoint reduction in hypertension (LIFE) study showed less new-onset atrial fibrillation (AF) in hypertensive patients receiving losartan- vs. atenolol-based t [...] Read more.Eran S. Zacks ... Richard B. DevereuxPublished: March 17, 2022 Explor Med. 2022;3:128–138
DOI: https://doi.org/10.37349/emed.2022.00079
This article belongs to the special issue Angiotensins—A Century of Progress -