Aim:
Among treatments for chronic non-cancer pain (CNCP), cannabinoid-based medicines (CBMs) have become extremely popular. Evidence remains modest and limited primarily to delta-9-tetrahydrocannabinol (THC) for neuropathic pain; nevertheless, the use of various CBMs, including cannabidiol (CBD) to treat neuropathic, nociceptive, and mixed pain has increased globally. This observational case-series assessed the impact of CBMs as a complementary treatment by pain mechanism and cannabinoid profile over three months.
Methods:
An analysis of patients with CNCP and treated with CBMs who consented to an ongoing registry was performed. Outcomes were patient-reported such as the Edmonton Symptom Assessment System-Revised, Brief Pain Inventory-Short Form, and 36-Item Short Form Health Survey. Data from patients with complete outcomes for baseline and 3-month follow-up was extracted. Characteristics of adverse drug reactions (ADRs), including a description of the suspected product were also assessed.
Results:
A total of 495 patients were part of this analysis (mean age = 56 years old; 67% women). At 3-month, the proportional use of THC:CBD balanced and THC-dominant products increased. Patients with neuropathic pain had higher pain-severity scores vs. nociceptive pain. In addition to patients with neuropathic pain, patients with nociceptive and mixed pain also reported improvements in pain severity and secondary symptoms such as anxiety, depression, drowsiness, fatigue, sleep disturbances, and overall, health-related quality of life. THC-dominant treatment is more likely to be recommended when pain is severe, whereas CBD-dominant is favored for less severe cases. ADRs were more frequent among cannabis-naive patients and included dizziness, headache, and somnolence among others.
Conclusions:
Findings suggest that CBMs can be effective for neuropathic as well as nociceptive and mixed pain. THC is more frequently recommended for neuropathic and severe pain. Future research on CBMs in pain management must include details of CBM composition, and pain mechanism and must consider potential ADRs.
Lucile Rapin ... Michael Dworkind
Aim:
Among treatments for chronic non-cancer pain (CNCP), cannabinoid-based medicines (CBMs) have become extremely popular. Evidence remains modest and limited primarily to delta-9-tetrahydrocannabinol (THC) for neuropathic pain; nevertheless, the use of various CBMs, including cannabidiol (CBD) to treat neuropathic, nociceptive, and mixed pain has increased globally. This observational case-series assessed the impact of CBMs as a complementary treatment by pain mechanism and cannabinoid profile over three months.
Methods:
An analysis of patients with CNCP and treated with CBMs who consented to an ongoing registry was performed. Outcomes were patient-reported such as the Edmonton Symptom Assessment System-Revised, Brief Pain Inventory-Short Form, and 36-Item Short Form Health Survey. Data from patients with complete outcomes for baseline and 3-month follow-up was extracted. Characteristics of adverse drug reactions (ADRs), including a description of the suspected product were also assessed.
Results:
A total of 495 patients were part of this analysis (mean age = 56 years old; 67% women). At 3-month, the proportional use of THC:CBD balanced and THC-dominant products increased. Patients with neuropathic pain had higher pain-severity scores vs. nociceptive pain. In addition to patients with neuropathic pain, patients with nociceptive and mixed pain also reported improvements in pain severity and secondary symptoms such as anxiety, depression, drowsiness, fatigue, sleep disturbances, and overall, health-related quality of life. THC-dominant treatment is more likely to be recommended when pain is severe, whereas CBD-dominant is favored for less severe cases. ADRs were more frequent among cannabis-naive patients and included dizziness, headache, and somnolence among others.
Conclusions:
Findings suggest that CBMs can be effective for neuropathic as well as nociceptive and mixed pain. THC is more frequently recommended for neuropathic and severe pain. Future research on CBMs in pain management must include details of CBM composition, and pain mechanism and must consider potential ADRs.
 Associations between methamphetamine and alcohol use disorder, suicidal ideation, and lowered quality of life in methamphetamine usersOpen AccessOriginal ArticleAim: There is a strong comorbidity between methamphetamine (MA) and alcohol use whereby MA use may contribute to increased alcohol consumption. This study aims to determine the associations betwe [...] Read more.Ketsupar Jirakran ... Rasmon KalayasiriPublished: June 30, 2023 Explor Med. 2023;4:409–420
Associations between methamphetamine and alcohol use disorder, suicidal ideation, and lowered quality of life in methamphetamine usersOpen AccessOriginal ArticleAim: There is a strong comorbidity between methamphetamine (MA) and alcohol use whereby MA use may contribute to increased alcohol consumption. This study aims to determine the associations betwe [...] Read more.Ketsupar Jirakran ... Rasmon KalayasiriPublished: June 30, 2023 Explor Med. 2023;4:409–420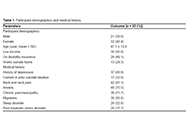 Exploring medical cannabis use in individuals with a traumatic brain injuryOpen AccessOriginal ArticleAim: Traumatic brain injury (TBI) is a common neurological condition, which can present with a wide range of neuropsychological symptoms. Treating this broad spectrum of symptoms represents a sig [...] Read more.Elizabeth N. R. Schjelderup ... Alasdair M. BarrPublished: June 30, 2023 Explor Med. 2023;4:393–408
Exploring medical cannabis use in individuals with a traumatic brain injuryOpen AccessOriginal ArticleAim: Traumatic brain injury (TBI) is a common neurological condition, which can present with a wide range of neuropsychological symptoms. Treating this broad spectrum of symptoms represents a sig [...] Read more.Elizabeth N. R. Schjelderup ... Alasdair M. BarrPublished: June 30, 2023 Explor Med. 2023;4:393–408 Molecular mechanism of electroacupuncture for improving perioperative complications with the guidance of enhanced recovery after surgeryOpen AccessReviewEnhanced recovery after surgery (ERAS) is a recommended surgical strategy at present, the core content is to reduce perioperative stress response and postoperative complications through perioperativ [...] Read more.Yu Mao, Lifang YangPublished: June 30, 2023 Explor Med. 2023;4:380–392
Molecular mechanism of electroacupuncture for improving perioperative complications with the guidance of enhanced recovery after surgeryOpen AccessReviewEnhanced recovery after surgery (ERAS) is a recommended surgical strategy at present, the core content is to reduce perioperative stress response and postoperative complications through perioperativ [...] Read more.Yu Mao, Lifang YangPublished: June 30, 2023 Explor Med. 2023;4:380–392 Cannabinoid-based medicines in clinical care of chronic non-cancer pain: an analysis of pain mechanism and cannabinoid profileOpen AccessOriginal ArticleAim: Among treatments for chronic non-cancer pain (CNCP), cannabinoid-based medicines (CBMs) have become extremely popular. Evidence remains modest and limited primarily to delta-9-tetrahydrocann [...] Read more.Lucile Rapin ... Michael DworkindPublished: June 30, 2023 Explor Med. 2023;4:363–379
Cannabinoid-based medicines in clinical care of chronic non-cancer pain: an analysis of pain mechanism and cannabinoid profileOpen AccessOriginal ArticleAim: Among treatments for chronic non-cancer pain (CNCP), cannabinoid-based medicines (CBMs) have become extremely popular. Evidence remains modest and limited primarily to delta-9-tetrahydrocann [...] Read more.Lucile Rapin ... Michael DworkindPublished: June 30, 2023 Explor Med. 2023;4:363–379 The impact of COVID-19 pandemic on diagnosis and management of gastrointestinal cancersOpen AccessReviewGastrointestinal (GI) cancer is one of the leading causes of death that affect many patients around the world. The coronavirus disease 2019 (COVID-19) pandemic significantly impacted our healthcare [...] Read more.Byung Soo Yoo ... David A. JohnsonPublished: June 28, 2023 Explor Med. 2023;4:356–362
The impact of COVID-19 pandemic on diagnosis and management of gastrointestinal cancersOpen AccessReviewGastrointestinal (GI) cancer is one of the leading causes of death that affect many patients around the world. The coronavirus disease 2019 (COVID-19) pandemic significantly impacted our healthcare [...] Read more.Byung Soo Yoo ... David A. JohnsonPublished: June 28, 2023 Explor Med. 2023;4:356–362 Association between coronavirus 2019 disease and pseudoneurological complaints: analysis of case-control dataOpen AccessOriginal ArticleAim: Pseudoneurological complaints (PNCs) are highly prevalent among the general population. Coronavirus disease 2019 (COVID-19) adversely influences such complaints in individuals who recovered [...] Read more.Mohammad Ali ... Tajnuva MehjabinPublished: June 28, 2023 Explor Med. 2023;4:343–355
Association between coronavirus 2019 disease and pseudoneurological complaints: analysis of case-control dataOpen AccessOriginal ArticleAim: Pseudoneurological complaints (PNCs) are highly prevalent among the general population. Coronavirus disease 2019 (COVID-19) adversely influences such complaints in individuals who recovered [...] Read more.Mohammad Ali ... Tajnuva MehjabinPublished: June 28, 2023 Explor Med. 2023;4:343–355 Type 2 diabetes mellitus and coronary artery stenosis: a risk pattern association studyOpen AccessOriginal ArticleAim: Cardiovascular diseases (CVD) are the leading cause of death globally. In the condition of type 2 diabetes mellitus (T2DM), the prevalence of CVD increase parallel with the rise of metabolic [...] Read more.Dharmsheel Shrivastav ... Vimal MehtaPublished: June 28, 2023 Explor Med. 2023;4:336–342
Type 2 diabetes mellitus and coronary artery stenosis: a risk pattern association studyOpen AccessOriginal ArticleAim: Cardiovascular diseases (CVD) are the leading cause of death globally. In the condition of type 2 diabetes mellitus (T2DM), the prevalence of CVD increase parallel with the rise of metabolic [...] Read more.Dharmsheel Shrivastav ... Vimal MehtaPublished: June 28, 2023 Explor Med. 2023;4:336–342 Vascular accesses: Which choice? Less is more, more or lessOpen AccessLetter to the EditorIn the context of in-hospital care management, the need for infusion therapies involves the choice of appropriate devices. Historically, there is no consensus about the preference for vascular acces [...] Read more.Regina Frontera, Mirko BaronePublished: May 31, 2023 Explor Med. 2023;4:333–335
Vascular accesses: Which choice? Less is more, more or lessOpen AccessLetter to the EditorIn the context of in-hospital care management, the need for infusion therapies involves the choice of appropriate devices. Historically, there is no consensus about the preference for vascular acces [...] Read more.Regina Frontera, Mirko BaronePublished: May 31, 2023 Explor Med. 2023;4:333–335 Effect of overweight and obesity on spirometric parameters in children and adolescent with asthmaOpen AccessOriginal ArticleAim: Being overweight and obesity are factors in the negative modification of bronchial asthma (BA). The mechanisms of the aggravating effect of obesity on the course of BA have not yet been fully determined, but include changes i [...] Read more.Regina N. Khramova ... Olga V. KhaletskayaPublished: May 30, 2023 Explor Med. 2023;4:323–332
Effect of overweight and obesity on spirometric parameters in children and adolescent with asthmaOpen AccessOriginal ArticleAim: Being overweight and obesity are factors in the negative modification of bronchial asthma (BA). The mechanisms of the aggravating effect of obesity on the course of BA have not yet been fully determined, but include changes i [...] Read more.Regina N. Khramova ... Olga V. KhaletskayaPublished: May 30, 2023 Explor Med. 2023;4:323–332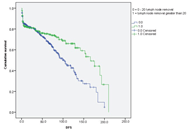 Effect of number of dissected lymph nodes on prognosis of patients with stage II and III colorectal cancerOpen AccessOriginal ArticleAim: There is a correlation between the number of resected lymph nodes (LNs) and survival as well as staging in patients with colorectal cancer (CRC). This cohort discussed the effect of the numb [...] Read more.Reihane Mokarian Rajabi ... Sayyideh Forough HosseiniPublished: May 30, 2023 Explor Med. 2023;4:314–322
Effect of number of dissected lymph nodes on prognosis of patients with stage II and III colorectal cancerOpen AccessOriginal ArticleAim: There is a correlation between the number of resected lymph nodes (LNs) and survival as well as staging in patients with colorectal cancer (CRC). This cohort discussed the effect of the numb [...] Read more.Reihane Mokarian Rajabi ... Sayyideh Forough HosseiniPublished: May 30, 2023 Explor Med. 2023;4:314–322