46 results in Exploration of Digestive Diseases
Latest
Sort by :
- Latest
- Most Viewed
- Most Downloaded
- Most Cited
Open Access
Original Article
GDF11 induces chemosensitization in human hepatocellular carcinoma cells by decreasing drug-efflux transporters
Natanael German-Ramirez ... Luis E. Gomez-Quiroz
Published: December 30, 2025 Explor Dig Dis. 2025;4:1005108

Open Access
Review
Diverticulitis—new evidence to share with patients
Nicholas B. D’Alessandro ... David A. Johnson
Published: December 24, 2025 Explor Dig Dis. 2025;4:1005107
This article belongs to the special issue Diverticulitis: Pathomechanism, Diagnosis and Treatment
Open Access
Review
CRISPR genome editing advances against gastric cancer
Mengmeng Zhang ... Xianguang Yang
Published: December 09, 2025 Explor Dig Dis. 2025;4:1005106

Open Access
Review
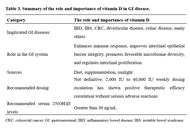
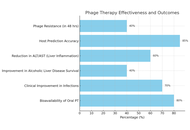
The therapeutic potential of bacteriophage therapy in liver cirrhosis: a comprehensive review of current evidence
Sarala Gudla ... Srijamya
Published: December 08, 2025 Explor Dig Dis. 2025;4:1005105
This article belongs to the special issue Gut Microbiota towards Personalized Medicine in Metabolic Disease
Open Access
Review
Pediatric cirrhosis: special consideration for its diagnosis and management
Guillermo Alejandro Costaguta, Fernando Álvarez
Published: December 07, 2025 Explor Dig Dis. 2025;4:1005104
This article belongs to the special issue Cirrhosis and Its Complications

Open Access
Case Report
Ixekizumab-associated severe Crohn’s in a patient without definitive immune-mediated inflammatory disease: case report and evidence-informed guidance for non-IBD clinicians
Taylor L. Spiewak ... Anish Patel
Published: December 01, 2025 Explor Dig Dis. 2025;4:1005103
Open Access
Editorial
Surveillance for cholangiocarcinoma in PSC: MRI, ERCP, both—or neither?
Vincenzo Giorgio Mirante
Published: November 26, 2025 Explor Dig Dis. 2025;4:1005102
This article belongs to the special issue Advances in Hepato-gastroenterology: Diagnosis, Prognostication, and Disease Stratification
Open Access
Review
Sex differences in alcohol-related liver disease, viral hepatitis, metabolic dysfunction-associated steatotic liver disease, and hepatocellular carcinoma
Amedeo Lonardo, Ayako Suzuki
Published: November 26, 2025 Explor Dig Dis. 2025;4:1005101

Open Access
Review
Neurotrophic signaling in liver cancers: mechanisms and potential therapeutic targets
Lorenzo Mainardi ... Chiara Raggi
Published: November 11, 2025 Explor Dig Dis. 2025;4:1005100
This article belongs to the special issue Fibrosis and Hepatobiliary Cancer

Open Access
Perspective
From spark to wildfire: how hyperferritinemia fans the flames of metabolic dysfunction-associated steatotic liver disease
Ralf Weiskirchen
Published: October 28, 2025 Explor Dig Dis. 2025;4:100599
This article belongs to the special issue Advances in Hepato-gastroenterology: Diagnosis, Prognostication, and Disease Stratification

Open Access
Review
Recent advances in Helicobacter pylori diagnosis, treatment, and management: a comprehensive review
Surbhi Dumra, Abhishek Ray
Published: October 21, 2025 Explor Dig Dis. 2025;4:100598
This article belongs to the special issue Helicobacter Pylori and Infection: Genomics, Diagnosis, Pathogenesis, Antibiotic Resistance, Microbiota, Cancer, Prevention and Therapeutics
Open Access
Review
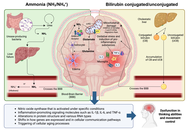
How the gut-liver axis shapes hepatic encephalopathy: mechanistic and therapeutic perspectives
Arnulfo E. Morales-Galicia ... Nahum Méndez-Sánchez
Published: October 14, 2025 Explor Dig Dis. 2025;4:100597
Open Access
Original Article
Multiple abnormalities of anorectal physiology co-exist with dyssynergia in patients with functional defecatory disorder—an observational study based on the London classification
Stephan Benny ... Noble Varghese Mathews
Published: October 11, 2025 Explor Dig Dis. 2025;4:100596

Open Access
Review
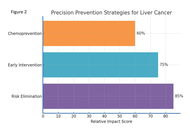
Precision prevention of liver cancer based on risk factors
Jian-Guo Chen
Published: September 29, 2025 Explor Dig Dis. 2025;4:100595
This article belongs to the special issue Prevention, Screening and Diagnosis for Primary Liver Cancer
Open Access
Original Article
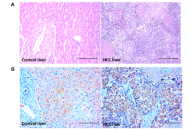
Elevated circulating pregnane X receptor as a novel diagnostic biomarker in hepatocellular carcinoma
Balasubramaniyan Vairappan ... Biju Pottakkat
Published: September 25, 2025 Explor Dig Dis. 2025;4:100594
This article belongs to the special issue Prevention, Screening and Diagnosis for Primary Liver Cancer
Open Access
Review
Insights of hepatitis A virus disease burden in Indian subcontinent: why urbanized localities are vulnerable to disease outbreaks?
Zahid Hussain ... Vivek Patel
Published: September 24, 2025 Explor Dig Dis. 2025;4:100593
This article belongs to the special issue Viral Hepatitis

Open Access
Mini Review
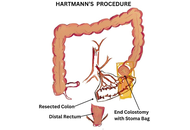
Surgical interventions: new approaches in diverticulitis treatment
Kaushal Yadav, Sagir Ahamed
Published: September 18, 2025 Explor Dig Dis. 2025;4:100592
This article belongs to the special issue Diverticulitis: Pathomechanism, Diagnosis and Treatment
Open Access
Original Article
Novel research in the field of non-invasive diagnostics of Helicobacter pylori utilizing a library of chemical piezoelectric sensors and portable devices
Tatyana Anatolievna Kuchmenko ... Arina Kopaeva
Published: September 14, 2025 Explor Dig Dis. 2025;4:100591
This article belongs to the special issue Helicobacter Pylori and Infection: Genomics, Diagnosis, Pathogenesis, Antibiotic Resistance, Microbiota, Cancer, Prevention and Therapeutics

Open Access
Review
PPARs in molecular pathogenesis and drug treatment of type 2 diabetes-related MASLD
Amedeo Lonardo, Ralf Weiskirchen
Published: September 02, 2025 Explor Dig Dis. 2025;4:100590
This article belongs to the special issue Nuclear Receptors and the Digestive Tract: from Molecular Physiology to Clinics via Pharmacology

Open Access
Review
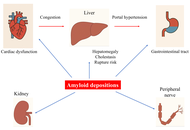
Amyloidosis and liver. Review.
Paul Carrier ... Véronique Loustaud-Ratti
Published: August 28, 2025 Explor Dig Dis. 2025;4:100589
Journal Information